
(source)
In the previous post in this series, we saw conclusive evidence that there has to this day not been “one single paper in which SARS-CoV-2 has been isolated and finally really purified,” and being that virus isolation and particle purification is the only means by which to positively identify a new virus, that, “In other words, the existence of SARS-CoV-2 RNA is based on faith, not fact.” Among the many studies alleging isolation of the novel ‘virus’, CDC researchers claimed in a paper published in June 2020 that, “we isolated virus,” all the way back at the end of January in fact, and subsequently “made the virus isolate available to the public health community,” and yet the CDC plainly stated in its PCR test “Instructions for Use” manual, in both July and December updates to the document, that “there are currently no quantified virus isolates available for use.”
This is because, contrary to the claims of the studies purporting to do so, the ‘virus’ was never actually isolated, and we looked at the admissions of four authors of 2020 papers “claiming discovery of a new coronavirus [who] concede they had no proof that the origin of the virus genome was viral-like particles or cellular debris, pure or impure, or particles of any kind,” and a fifth admission is included in this post. Not a single one of the genomes being passed off as ‘SARS-CoV2’ was obtained through end-to-end sequencing of a purified virus particle, or particle of any kind obtained from any patient sample for that matter, but rather computer-generated, as was openly admitted in the flawed Drosten-Corman study tasked by the World Health Organization (WHO) with establishing and validating the global PCR detection protocol used for Covid ‘diagnosis’ to this day, and as even the ‘fact-checkers’ concede in regards to the genome sequence used by the CDC and which PCR tests in the US have been calibrated to detect. As was also shown, Pfizer similar used a computer-generated ‘virus’ genome for its ‘vaccine’ DNA template, and not viral RNA from a virus isolate taken directly from a patient, as UK MHRA admitted.
In this post we will take a closer look at the establishment ‘isolation’ process utilized by the CDC researchers falsely alleging isolation of the virus, how the viral genome being passed off as ‘SARS-CoV2’ was constructed, the colossal PCR fraud responsible for giving rise to and perpetuating this illusion, and the CDC’s own research indicating that the alleged virus is neither cytopathic nor infective to human cells, which amounts to compelling evidence that the ‘virus’, if it exists as CDC and the whole of the medical establishment claims, cannot be the true cause of ‘Covid-19’.
‘SARS-CoV2’ a computer-generated ‘virus’
Despite their claims, the CDC did not actually “isolate virus,” as the ‘isolation’ process described in the June, 2020 CDC study which purported to do so - “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States” - clearly reveals. Instead, they take a patient sample containing various sources of genetic material and only presumed to contain virus, and stick it straight into a mixture of monkey kidney (“Vero”) cells, fetal bovine serum and antibiotics, where they then culture the whole sample until cell damage is observed, these cytopathic effects passed off as ‘proof’ there’s a ‘virus’ hidden somewhere in the mixture causing this damage, at which point the dying cells are scraped clean and this removed material ‘identified’ as the ‘virus’ being ‘isolated’ from the sample. This material is then labelled the “isolate” from which the ‘viral RNA’ (nucleic acids) would be “extracted” and “amplified,” and then sequenced and cultured as virus.
At no point during this process, however, was the alleged virus actually isolated from all of the other genetic material and other contaminates contained within the sample, and the process of culturing the sample in monkey kidney cells only serves to further contaminate it rather than aid in the purification of any alleged virus that may or may not be contained therein, particularly given the addition of antibiotics to the genetic ‘soup’.
Only after the isolation process is complete can researchers positively identify the remaining identical particles as the virus in question, and only then can the virus be sequenced and cultured; culturing alleged virus before it is purified is not a form of virus isolation, and it does not result in a virus isolate but rather an impure “isolate material” containing genetic material which may or may not contain virus or viral fragments, from which nucleic acids said to be the virus, and not whole particles, are then extracted, or fished out of the ‘soup’ with a selected PCR primer thought to match the viral genome sequence.
This is exactly the kind of monkey business referenced in the opening quote of this post. Dr. Andrew Kaufman does a great job of breaking down this convoluted process into laymen’s terms in his step-by-step analysis of the CDC’s method of ‘isolation’ (here). Suffice it to say that this extremely flawed process does not result in isolated virus or purified virus particles, and neither do the cytopathic effects observed in the cells prove the existence of virus in the contaminated genetic ‘soup’; in fact, the antibiotics or other toxins utilized in this process can cause the observed cell damage, and in this case the specific antibiotics used do just so happen to be toxic to kidneys and are being applied to a monkey kidney cell culture! Why it is deemed necessary to add a chemical concoction to the cell culture in this ‘isolation’ process is beyond me, but choosing a substance known to be toxic to the very cells the sample is being cultured in sure would be a convenient way of engineering a scenario in which cytopathic effects are consistently observed in every cultured sample...
And although this process is passed off as ‘isolation’, it is the next step of sequencing that is really considered to be the act of ‘isolating’ the ‘virus’, as Prof. Karen Mossman, in charge of the research team at McMaster University which undertook the ‘isolation’ of the ‘virus’ in Canada, explains in her article - “I study viruses: How our team isolated the new coronavirus to fight the global pandemic”:
Since specimens from patients are also likely to contain other viruses, it is critical to determine if a virus growing in the culture is really the target coronavirus. Researchers confirm the source of infection by extracting genetic material from the virus in culture and sequencing its genome.
They compare the sequence to known coronavirus sequences to identify it precisely. Once a culture is confirmed, researchers can make copies to share with colleagues.
These “known coronavirus sequences” used to ‘identify’ the extracted genetic material as ‘SARS-CoV2’, however, are all based upon computer-generated sequences that are in turn based upon the original Wuhan strain sequence derived from patient samples in which the particles alleged to be virions were admittedly never purified or sequenced from end-to-end. And without a single complete genome sequence of any of the particles in question, the claim that this method is a valid means of “precisely” identifying the ‘virus’ is both laughable and thoroughly unscientific. It is impossible to positively identify any genetic material as part of a virus which itself has never been identified.
As the authors of “Phantom Virus: In search of Sars-CoV-2” explain:
As the virus you are looking for is new, there are clearly no ready genetic primers to match the specific fraction of the new virus; so you take [PCR] primers that you believe may be closer to the hypothesised virus structure, but it’s a guess, and when you apply the primers to the [cultured] supernatant broth, your primers can attach to any one of the billions of molecules present in it, and you have no idea that what you have thus generated is the virus you are looking for.
The next step in the CDC process reveals just how the type of “full length RNA” genome sequence used in place of a quantified virus isolate in the PCR detection regimen is manufactured. Rather than performing complete end-to-end sequencing of purified virus particles or particles of any kind, the CDC “Whole Genome Sequencing” process involves taking just 37 base genome pairs selected based on a reference sequence that in turn did not come from purified virus particles to create the “full genome” of over 30,000 pairs, using nucleic acids extracted from the non-purified “isolates” described above.
We designed 37 pairs of nested PCRs spanning the genome on the basis of the coronavirus reference sequence (GenBank accession no. NC045512). We extracted nucleic acid from isolates and amplified by using the 37 individual nested PCRs.
Then, as journalist Makia Freeman notes,
Interestingly enough, in the next paragraph, the CDC scientists say they used “quantitative PCR” for further analysis/construction, which goes against what Kary Mullis, the inventor of PCR, once said – namely that “quantitative PCR is an oxymoron” since PCR is inherently a qualitative technique not a quantitative one.”
That this process does not result in purified virus was admitted by an author of one of the studies similarly alleging isolation of the virus and published in The Medical Journal of Australia, Sharon R. Lewis et al.: "The nucleic acid extraction was performed on isolate material recovered from infected cells. This material was not centrifuged, so was not purified through sucrose gradient to have a density band as such. The EM images were obtained directly from cell culture material.”
This presents a real problem, even for those who maintain that virus isolation cannot be performed prior to sample culturing, as centrifugation is the key step in the process during which isolation of the virus is actually achieved.
This process is not in dispute, and is also detailed in college textbooks such as Microbiology, an open source textbook the publishers note “aligns with the curriculum guidelines of the American Society for Microbiology.” Under the heading “Isolation of Viruses,” we read:
Unlike bacteria, many of which can be grown on an artificial nutrient medium, viruses require a living host cell for replication. Infected host cells (eukaryotic or prokaryotic) can be cultured and grown, and then the growth medium can be harvested as a source of virus. Virions in the liquid medium can be separated from the host cells by either centrifugation or filtration.
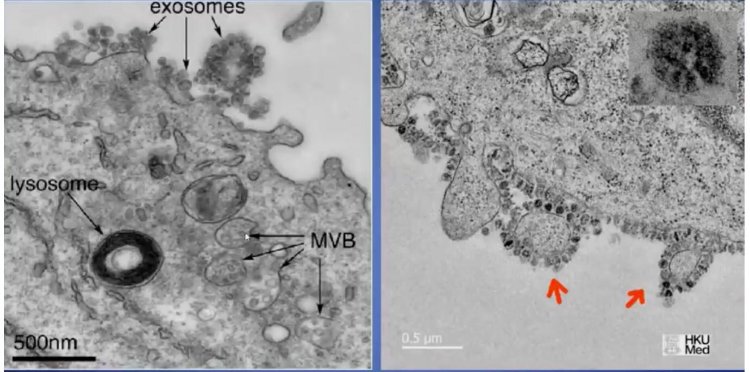
Further complicating the matter is the fact that centrifugation - an essential step in the virus isolation process admittedly skipped by a number of institutions performing the establishment method of ‘isolation’ - is alone likely an insufficient means of achieving complete particle purification. The reason for this being the existence of extracellular vesicles (EVs) produced by our bodies, perhaps the most prevalent of these being exosomes, as the scientific literature informs us that these beneficial nanoparticles so resemble viruses that they are often entirely indistinguishable from viruses under the microscope. As explained in “The Role of Extracellular Vesicles as Allies of HIV, HCV and SARS Viruses” published in the journal Viruses in May 2020:
Nowadays, it is an almost impossible mission to separate EVs and viruses by means of canonical vesicle isolation methods, such as differential ultracentrifugation, because they are frequently co-pelleted due to their similar dimension,...
Given that exosomes, like viruses, also contain nucleic acids, proteins, and lipids, and a comparison of electron micrographs of exosomes and the particles passed off as ‘SARS-CoV2’ reveal they can be of the same size and structure, “it is therefore plausible to believe that, in the large sea of particles contained in the supernatant of the COVID-19 patient’s broncho-alveolar fluid, what is taken to be SARS-CoV-2 is but an exosome,” as the authors of “Phantom Virus” note.
That exosomes would consistently be present in Covid patient samples is certainly possible, as one of their primary functions is to aid the body’s natural response to illness during battle with disease, as extensive medical research has found.
Indeed, a number of doctors and scientists have proposed this theory, and have concluded that what is taken to be viral particles responsible for causing disease in Covid patients are in fact beneficial exosomes which are instead present as a result of that disease. Thus the importance of next proving that particles isolated from patient samples are in fact the cause of that disease once the virus has been isolated, which in this case was never done.
In short, the ‘isolation’ process described by the CDC does not result in purified particles that can be sequenced, and this is why, despite claiming to have isolated the virus and then made that virus isolate available, would later write in its PCR “Instructions for Use” document, that “there is currently no quantified isolate available,” and it is also why the “full RNA genome” sequence of ‘SARS-CoV2’ was computer-generated from just a few genome pairs rather than obtained through end-to-end sequencing of an isolated, purified virus specimen.
In October 2020, in “Only poisoned monkey kidney cells grew the virus,” Dr. Tom Cowan explains the inherently flawed and fraudulent nature of this process as a means of ‘identifying’ a novel virus.
To me, this computer-generation step constitutes scientific fraud. Here is an equivalency: A group of researchers claim to have found a unicorn because they found a piece of a hoof, a hair from a tail, and a snippet of a horn. They then add that information into a computer and program it to re-create the unicorn, and they then claim this computer re-creation is the real unicorn. Of course, they had never actually seen a unicorn so could not possibly have examined its genetic makeup to compare their samples with the actual unicorn’s hair, hooves and horn.
The researchers claim they decided which is the real genome of SARS-CoV-2 by “consensus,” sort of like a vote. Again, different computer programs will come up with different versions of the imaginary “unicorn,” so they come together as a group and decide which is the real imaginary unicorn.
This consensus is in large part reached by way of reliance upon the original Wuhan strain sequence and the entirely computer-generated Drosten sequence not even built upon genetic material taken from a patient sample as the foundational ‘virus’ templates against which all future sequences are compared, and this forms the ‘gold standard’ of virus identification in the Covid Clown World of 2020/2021!
As the authors of “Phantom Virus” put it, “they did not analyse the whole genome, but instead took some sequences found in the cultures, claimed without proof that they belonged to a new specific virus, and then made some sort of a genetic computer puzzle to fill up the rest.”
As can be clearly seen, ‘SARS-CoV2’ is quite literally a theoretical virus, a phantom virus never proven to exist. And in light of this unscientific process of chasing an invisible phantom virus, Donald Trump’s declaration that we are at war against an “invisible enemy” takes on real meaning, because truth be told, actual viruses haven’t been invisible since the invention of the electron microscope decades ago. But once the public has been convinced that the world is haunted by this phantom virus, it is only natural that they would accept as valid any means of ‘detecting’ the invisible enemy the authorities introduced, so long as they were assured it could truly identify the ‘enemy’, in much the same way ghost hunters have full confidence in their ghost detection devices.
PCR Fraud, mechanism of mass deception
The inherent flaws of PCR as a disease diagnostic have been well documented, and equally problematic is PCR use for virus identification, particularly when it comes to the identification of new viruses, such as the novel coronavirus we are allegedly here dealing with, and which PCR played a principle, key role in the supposed identification of.
“Scientists are detecting novel RNA in multiple patients with influenza or pneumonia-like conditions, and are assuming that the detection of RNA (which is believed to be wrapped in proteins to form an RNA virus, as coronaviruses are believed to be) is equivalent to isolation of the virus. It is not,” David Crowe explains in his paper, “Flaws in Coronavirus Pandemic Theory.”
Interestingly enough, scientific literature detailing the difficulty of novel virus identification with PCR had already been published in medical journals for well over a decade before the arrival of ‘Covid19’.
In “Identification of a new human coronavirus,” published in Nature on April 4, 2004, the authors state that: “Major difficulties are encountered ... when searching for new viruses,” noting that "the identification of unknown pathogens using molecular biology tools is difficult because the target sequence is not known so that PCR-specific initiators cannot be designed.”
And yet that is exactly the process by which the medical authorities ‘identified’ this new ‘virus’, by designing PCR initiators (partial RNA sequences) thought to be unique to ‘SARS-CoV2’ before its identity had actually been ascertained through complete end-to-end genome sequencing of purified particles, or any particles for that matter, pure or impure, viral or not.
At the same time the paper,“Characterization and Complete Genome Sequence of a Novel Coronavirus, Coronavirus HKU1, from Patients with Pneumonia,” published in the Journal of Virology in January 2005, incredibly opens with the following words: "Despite extensive research in patients with respiratory tract infections, no microbiological cause has been identified in a significant proportion of patients. RNA is extracted from non-purified cultures.”
Such a process will by now be all too familiar to readers, and the acknowledgment that RNA extracted from non-purified cultures does not result in the identification of an infectious disease cause in patients is quite telling, considering the institutions which have done just this when it comes to Covid patient samples pass it off as proof of the existence of ‘SARS-CoV2’ as the cause of ‘Covid19’...
In light of such statements, it is not particularly surprising then, that in the first study alleging isolation of the ‘virus’ conducted in China and published in the New England Journal of Medicine on February 20, 2020, we can read the remarkable admission that:
“Further development of accurate and rapid methods to identify unknown respiratory pathogens is still needed … our study does not fulfill Koch’s postulates.”
The problems inherent with attempts at rapidly identifying new respiratory pathogens noted in the wake of the initial SARS outbreak have still not been resolved, and yet the world relied solely on these flawed rapid identification methods to establish existence of ‘SARS-CoV2’ and ‘identify’ it as the cause of disease in patients. Notably, the study itself did not establish the ‘virus’ to be the definitive cause of disease in the 17 Pneumonia patients in Wuhan from which the samples were taken, the primary function of Koch’s postulates.
Similarly, the authors of the paper entitled “Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China,” published in The Lancet on February 15, 2020, made the honest admission that, “we did not perform tests for detecting infectious virus in blood,” and yet go on to repeatedly refer to the 41 PCR-positive cases (out of 59 total) as, “41 patients... confirmed to be infected with 2019-nCoV,” revealing the inherently dogmatic nature of the Covid narrative and the tremendous faith in PCR held by so many in the scientific/medical establishment. This faith is both scientifically unsound and can have disastrous results, as history clearly demonstrates.
For those familiar with the very real documented history of reliance on PCR testing giving birth to very unreal pseudo epidemics, as occurred in Dartmouth in 2007 when, as a New York Times report headlined the story, “Faith in Quick Test Leads to Epidemic That Wasn’t,” red flags that something wasn’t right with the ‘pandemic’ narrative should have been immediately set off left and right when all of the establishment talking heads in unison began endlessly and religiously repeating the new mantra - “Test, test, test.” / “Testing, testing, testing.” - as they rolled out millions of PCR ‘diagnostic’ test kits around the world.
The world was being asked to put its faith in a test that experts had warned, based on the test’s role in producing the nonexistent whooping cough ‘epidemic’ of 2007, would eventually lead to the declaration of similar pseudo epidemics in the future, a big “problem” that was naturally “going to become more common” if PCR remained the choice method for detection and diagnosis of infectious diseases.
Now, as they look back on the episode, epidemiologists and infectious disease specialists say the problem was that they placed too much faith in a quick and highly sensitive molecular test [PCR] that led them astray.
As NYT candidly admitted, when it comes to PCR, “their very sensitivity makes false positives likely, and when hundreds or thousands of people are tested, as occurred at Dartmouth, false positives can make it seem like there is an epidemic,” even when there isn’t one.
Of course, that leads to the question of why rely on them at all. “At face value, obviously they shouldn’t be doing it,” Dr. Perl said.
And yet in 2020, health authorities around the world insisted with a straight face that getting the ‘pandemic’ under control would be best accomplished by tracking infections and spread of disease (‘contact tracing’) through the indiscriminate testing of as many millions of people as possible, as quickly as possible, with the inherently flawed PCR test; admittedly problematic just years earlier, now being universally hailed as the “gold standard” of novel virus identification and ‘Covid19’ diagnosis.
So “why rely on them at all?” One obvious reason would be for purposes of engineering a manufactured ‘pandemic’ that wasn’t, and there would certainly also be a profit motive for test manufacturers to pressure authorities to do the very thing experts had admitted they “obviously shouldn’t be doing.”
The testing mania began as soon as PCR ‘diagnostic’ kits were authorized for use, early Spring here in the US, and we must logically conclude that those introducing PCR as the global standard for coronavirus identification and Covid ‘diagnosis’ are either the most incredibly incompetent conglomerate of ‘experts’ on the face of the earth, who ignorantly failed to heed the clear warning signs of the past, or they were well aware of exactly what they were doing and intentionally introduced PCR as the primary mechanism by which to engineer a Plandemic. The PCR testing standards being used seem to clearly indicate that the latter is the more likely scenario.
That PCR ‘diagnostic’ kits packaged in boxes with disclaimers such as, “Not for use in diagnostic procedures,” were nevertheless being rolled out for wide-scale use as the primary and in many cases sole method of Covid diagnosis was another huge red flag indicative of the fraudulent nature of the testing campaign that would ensue.
Government agencies put out their own disclaimers admitting as much, albeit in round about ways, such as those contained in the CDC PCR test “Instructions for Use” document, which states that: “Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms,” and also: “This test can not rule out diseases caused by other bacterial or viral agents.”
Or the one made by the Australian government: “The reliability of COVID-19 tests is uncertain due to the limited evidence base…There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.”
Despite the myriad of disclaimers all but admitting that these tests are completely worthless, they were yet at the very same time universally declared to be the “gold standard” of coronavirus identification, even while there was no gold standard against which to measure the test’s specificity (accuracy) - a virus isolate from which a complete end-to-end genome sequence could be procured - testament to the unscientific and dogmatic nature of the clown show that ensued.
There are numerous inherent problems with the ongoing PCR testing campaign, not the least of which being that the ‘virus’ the tests are designed to detect is a pieced together, computer-engineered theoretical ‘Frankenstein’ virus - a man-made creation. Making matters worse, the tests are not actually calibrated to identify even this hypothetical virus, but rather only a very tiny fragment of viral RNA, a partial genetic sequence consisting of a mere 8-32 base pairs (PCRs) of a ‘virus’ containing over 30,000 such strands. In other words, even if the computer generated pseudo virus were an accurate representation of the alleged virus said to be found and isolated in dozens of patient samples, the PCR tests are still only looking for about 0.08% of the genetic material of that virus!
This is extremely problematic because such a minuscule partial genetic sequence is naturally shared by a whole host of other viruses and life forms, including the human genome itself, which could certainly help to account for why, during widespread testing of the general public, the majority of positive test results are labelled ‘asymptomatic infections’, with millions of people who aren’t sick being counted among ‘confirmed’ Covid cases.
Additionally, the partial genetic sequence being identified in samples differs from test to test, based upon the particular ‘strain’ sequence utilized and the specific partial sequence of that ‘strain’ which the PCR test is actually primed to identify, making the global ‘standard’ of virus identification very non-standardized indeed. The inherent problems of the testing standard are well summarized in the great article published by the Spanish health journal Salud in November 2020, entitled “Frauds and falsehoods in the medical field”.
The genetic sequences used in PCRs to detect suspected SARS-CoV-2 and to diagnose cases of illness and death attributed to Covid-19 are present in dozens of sequences of the human genome itself and in those of about a hundred microbes. And that includes the initiators or primers, the most extensive fragments taken at random from their supposed “genome” and even the so-called “target genes” allegedly specific to the “new coronavirus”. The test is worthless and all “positive” results obtained so far should be scientifically invalidated and communicated to those affected; and if they are deceased, to their relatives. Stephen Bustin, one of the world’s leading experts on PCR, in fact says that under certain conditions anyone can test positive!
We have been warning you since March: you cannot have specific tests for a virus without knowing the components of the virus you are trying to detect. And the components cannot be known without having previously isolated/purified that virus. Since then we continue to accumulate evidence that no one has isolated SARS-CoV-2 and, more importantly, that it can never be isolated.
Although this should be alarming, it is not particularly surprising, given that PCR is inherently incapable of identifying viruses, or diagnosing disease for that matter, as Kary Mullis, the award winning Nobel laureate who invented the revolutionary PCR technology, made quite clear. (1, 2)
“Although there is a common misimpression that the viral load tests actually count the number of viruses in the blood, “these tests cannot detect free, infectious viruses at all; they can only detect proteins that are believed, in some cases wrongly, to be unique to” any given virus, John Lauritsen explained in a 1996 article published in the New York Native. ”The tests can detect genetic sequences of viruses, but not viruses themselves.”
A Reuters ‘fact-check’ was forced to admit that this understanding may indeed be “a fair reflection of Mullis’ views,” because indeed it is. It is thus extremely relevant to the discussion of PCR tests now being used to “detect genetic sequences” that are “believed” (or at least said), “sometimes wrongly,” to be unique to a new ‘virus’ that still to this day hasn’t been isolated and from which a full genome sequence has yet to be obtained, particularly when such a small, incomplete sequence is being identified.
The only valid means of detecting actual viruses in patient samples is under an electron microscope; and so it is important to note, as discussed in my previous post, that the electron micrographs of the alleged ‘SARS-CoV2’ particles, admittedly not purified, which were provided in the Chinese study alleging initial isolation of the virus, reveal such a wide ranging size of alleged virus particles that they could not possibly all be the particles of a single novel virus. In typical Covid Clown Show fashion, the Wikipedia entry on coronavirus was eventually changed, likely to address this problem, to state the impossible as ‘fact’: “Each SARS-CoV-2 virion has a diameter of about 50 to 200 nm”.
This absurd statement is akin to claiming that your pet dog ranges from 50 to 200 pounds depending on where you find him; and while it is true that dogs vary greatly in size depending on breed, and there is even a slight size variance of individual dogs among each particular breed - border collies, for example, tend to range from 35 to 50 pounds - it is utterly nonsensical to assert that my individual border collie’s size varies so much that she could one day be triple or even double the size she was the day before!
But even if one is willing to accept such absurdity as scientific ‘fact’, and believes that ‘SARS-CoV2’ has been isolated and identified as the cause of Covid through the flawed establishment isolation process, and that the particles identified in patient samples are in fact this new virus, the PCR testing regimen still remains highly problematic, arguably criminally fraudulent, and definitely an extraordinarily inaccurate means of detecting this ‘virus’ in patient samples, due to the excessively high rate of false positives expected as the tests are used.
PCR tests work by amplifying patient samples with a certain number of cycles, each cycle further amplifying the sample, with the cycle threshold (CT) used determining the level of amplification. And as has been widely acknowledged, the PCR cycle used can largely determine the number of false positives produced, as over-cycling will naturally result in a high rate of false positives, with anything over a CT of about 29 resulting in an extremely high rate of false positives, and anything over 35 completely useless, churning out a near-100% rate of positive test results.
For example, one study found that at a cycle threshold of 30, the tests would produce a 70% rate of false positives, with a cycle threshold of 35 producing a 97% rate of false positives.
Dr. Fauci himself has publicly acknowledged this reality, that any CT over 34 is essentially meaningless in determining virus-positivity, and this is so well established in fact, that he explained all the way back in July 2020 that it was becoming an industry standard.
“It is evolving into somewhat of a standard that if you get a cycle threshold of 35 or more, the chances of it being replication-competent are minuscule,” Fauci said in the video conference linked above, adding that, “you almost never can culture virus from a 37 threshold cycle…even 36…it’s just dead nucleoids, period.”
At these levels of extreme amplification, the PCR tests will no longer be detecting genetic material of live virus but rather minuscule amounts of dead nucleoids in the sample resulting in a positive test result.
A month later in August, a New York Times investigation found that in the US, “Most tests are set at 40. Some at 37.” In the same piece, the Times also reported that these cycle thresholds can be expected to produce a 90% rate of false positives.
I’ll let readers do the math, but it doesn’t take a genius to see what the result of widespread testing of millions of people at these cycles will be. If there was one easy way to create the illusion of a pandemic that didn’t exist, regardless of whether a novel coronavirus had emerged or not, this would be it.
Many will be tempted to chalk this universal disregard of the industry testing standard up to incompetence, although this is a difficult argument to make in light of the fact that the leading coronavirus ‘expert’ himself is admittedly aware of the impact the use of PCR tests set at these cycles will have on the accuracy of Covid ‘case’ counts, and it is difficult to believe that prominent health officials like Fauci are unaware of the testing ‘standard’ being used by labs across the country (and Europe, for that matter), especially given that even the New York Times has reported on it.
That this is rather a colossal fraud being willfully perpetrated against the American public is confirmed by the fact that the CDC has since revealed that it is well aware of this problem, and yet has not acted to rectify it. In April, 2021, in a quiet update of its guidance for “COVID-19 vaccine breakthrough case investigation”, the CDC advised that: “Clinical specimens for sequencing should have an RT-PCR Ct value ≤28."
When ‘breakthrough cases’ among the ‘fully vaccinated’ began to stack up in the Spring, the CDC “suddenly discovered the power of cycle thresholds on PCR testing in determining whether the positive results are real or meaningful,”, and was compelled to immediately issue guidance in accordance with this understanding in order to reduce the number of false positives when it comes to ‘breakthrough cases’, but not when it comes to Covid ‘cases’ in the unvaccinated. That the CDC is aware of the problem of high PCR CTs and that labs are using these CTs is evidenced by this guidance, which in turn is evidence that the agency is knowingly and actively helping to perpetuate the Covid illusion, and not simply ignorant of this mechanism of over-inflating national Covid case counts.
If it wasn’t clear before the issuance of this guidance, that this PCR testing regimen constitutes fraud and not incompetence is now undeniable. Dr. Fauci, the New York Times, and the CDC are all well aware of the power of cycle thresholds to determine the number of false positives and thus the number of total recorded Covid ‘cases’ regardless of disease prominence, and yet this unscientific PCR testing regimen has continued in the name of ‘science’ for nearly two years now, without the medical authorities taking steps to establish testing protocols in alignment with the “industry standard” that would at least ensure relatively ‘accurate’ test results according to the framework of those operating under the assumption that the PCR tests are actually detecting RNA sequences of a novel coronavirus that both exists and causes ‘Covid-19’.
But the problem doesn’t end there, as even if the tests are not producing an excessive number of false positives due to over-cycling, and assuming the sequences they detect are actually indicative of the presence of virus, it must be expected that there will still be quite a high rate of false positives, as even the White House Coronavirus Task Force coordinator Deborah Birx stated in a 2020 press conference, revealing that government officials at the highest levels of the medical establishment are well aware that these tests are known to be capable of producing highly inaccurate results. In fact, Birx cited an expected 50% rate of false positives in a scenario where 1% of the population is infected using a test that is 99% specific (unrealistically high).
She says:
If you have 1% of the population infected and you have a test that is only 99% specific, then if you find a positive, then 50% of time it will be a real positive and 50% of time it won't be.
(Segment starts at 52m37s)
That the PCR tests are not 100% specific is elsewhere also admitted by Birx: “None of our tests are 100 percent sensitive and specific,” she noted.
If 50% of the positive test results are admittedly actually negative with a highly specific (accurate) test that is properly cycled, we have a very serious problem with the Covid case count, indeed. How this could be considered the ‘gold standard’ of Covid diagnosis in light of all of the admissions illuminating the inaccurate nature of these tests made by the experts, even under the most ideal conditions, is beyond me. However, it is entirely unrealistic that these tests could actually be 99% specific, and are far more likely to have only about 80-85% specificity (1), (2).
And as one researcher investigating the false positive prevalence based on Birx’s admissions noted:
Reduce to a more realistic test specificity of 85% (15, 85), and sensitivity 90%, prevalence 1%...
Then you get:
True positives: 5.71 = 6%
False positives: 100 - 6 = 94%
Over 90% are wrong results!
Because the test was developed using a test-tube with 100% virus prevalence as the standard, then as prevalence INCREASES (more true cases in population), the test becomes MORE reliable (but not by much):
If California has, say, 5% prevalence, then above calc (85% specificity) becomes:
True positives: 24%
False positives: 100 - 24 = 76%
76% of positive tests would be FALSE and wrong - about three quarters are wrong.
The link above contains additional analysis, links, and calculators used to achieve these numbers, so you can double check the math for yourself. But, as even NPR has acknowledged (in regards to antibody tests, but equally applicable to PCR): "If you used a test with 90% specificity in a population in which only 1% of the people have it...more than 90% of the positive results would be false positives."
So depending on disease prevalence, and forgetting the problem of widespread over-cycling, the PCR tests are still realistically producing false positives at a rate of about 75-94%! A 94% rate of false positives aligns with CDC data indicating that only 6% of deaths attributed to Covid had the disease listed as the sole cause of death, with an average of 2.5 co-morbidities listed on the death certificates of 94% of these deceased ‘Covid-19’ patients. These ‘co-morbidities’ could easily be the primary causes of death, and all of these patients in fact simply listed as Covid deaths as a result of false positive test results.
In any event, no matter how you slice it, even if this virus exists and is the cause of disease labelled ‘Covid-19’, all of the evidence indicates that a good 90% or more of ‘confirmed’ cases are in fact false positives and thus not in reality Covid cases at all, testament to the incredibly fraudulent nature of this PCR testing campaign.
CDC researchers, however, were not even able to demonstrate that their ‘isolated’ virus was infective or damaging to human cells, and the complete lack of evidence indicating that ‘SARS-CoV2’, if it exists, is the cause of ‘Covid-19’, further reduces the entire virus narrative to complete absurdity.
No evidence ‘SARS-CoV2’ is a cause of disease further reduces virus narrative to absurdity
Given that cytopathic effects observed in cell culture was the primary means of identifying the so-called virus in patient samples in the first place, the fact that CDC researchers were entirely incapable of producing any of these cytopathic effects when introducing their ‘virus isolate’ to human cells is an astonishing discovery, and it is astounding that in the wake of such findings, the agency would continue to insist that this ‘virus’ is the known cause of ‘Covid-19’ according to the ‘science’. These findings were described in the very same study detailing the agency’s isolation process, and the relevant portion of the study reads:
…we examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549), human liver cells (HUH7.0), and human embryonic kidney cells (HEK-293T), in addition to Vero E6 and Vero CCL81 cells. We also examined an available big brown bat kidney cell line (EFK3B) for SARS-CoV-2 replication capacity. Each cell line was inoculated at high multiplicity of infection and examined 24 h postinfection … No CPE [cytopathic effect] was observed in any of the cell lines except in Vero cells, which grew to >107 PFU at 24 h postinfection. In contrast, HUH7.0 and 293T cells showed only modest viral replication, and A549 cells were incompatible with SARS-CoV-2 infection. These results are consistent with previous susceptibility findings for SARS-CoV and suggest other common culture systems, including MDCK, HeLa, HEP-2, MRC-5 cells, and embryonated eggs, are unlikely to support SARS-CoV-2 replication. In addition, SARS-CoV-2 did not replicate in bat EFK3B cells, which are susceptible to MERS-CoV.
The ‘virus’ was not damaging to any of the three human tissue cultures, demonstrating under lab conditions that it is not capable of producing disease in humans! This alone destroys the entire virus narrative. But it was also entirely unable to infect one of the human tissue cultures, and had only modest replication in the other two, suggesting an inability to infect human cells at all, and the study authors go on to write that other common human cultures are “unlikely to support SARS-CoV-2 replication,” meaning ‘SARS-CoV2’ will not infect them either! And yet the public has been endlessly fearmongered for nearly two years with the story of a highly infectious and incredibly dangerous virus.
Dr. Cowan summarizes these findings as follows:
What does this language actually mean, and why is it the most shocking statement of all from the virology community? When virologists attempt to prove infection, they have three possible “hosts” or models on which they can test. The first is humans. Exposure to humans is generally not done for ethical reasons and has never been done with SARS-CoV-2 or any coronavirus. The second possible host is animals. Forgetting for a moment that they never actually use purified virus when exposing animals, they do use solutions that they claim contain the virus. Exposure to animals has been done once with SARS-CoV-2, in an experiment that used mice. The researchers found that none of the wild (normal) mice got sick. In a group of genetically modified mice, a statistically insignificant number lost some fur. They experienced nothing like the illness called Covid 19.
For those who did not read my previous piece, it is worth noting that this inability to produce disease in animals upon infection with the ‘virus’ is in stark contrast to the influenza filtrate of the 1933 influenza virus isolation project, which clearly seems to have caused disease in ferrets, as, upon infection, the animals developed symptoms closely matching those in the human patients from which the isolated samples were taken. Maybe ‘SARS-CoV2’ is in fact an infectious disease-causing virus with the sole symptom being sudden hair loss, as the fur loss among infected mice would indicate, and this could explain the bizarre sudden hair loss observed among a number of ‘long-haul Covid’ patients, but of course cannot account for the myriad of other symptoms attributed to the disease...
Dr. Cowan continues:
The third method virologists use to prove infection and pathogenicity — the method they most rely on — is inoculation of solutions they say contain the virus onto a variety of tissue cultures. As I have pointed out many times, such inoculation has never been shown to kill (lyse) the tissue, unless the tissue is first starved and poisoned.
The shocking thing about the above quote is that using their own methods, the virologists found that solutions containing SARS-CoV-2 — even in high amounts — were NOT, I repeat NOT, infective to any of the three human tissue cultures they tested. In plain English, this means they proved, on their terms, that this “new coronavirus” is not infectious to human beings. It is ONLY infective to monkey kidney cells, and only then when you add two potent drugs (gentamicin and amphotericin), known to be toxic to kidneys, to the mix.
My friends, read this again and again. These virologists, published by the CDC, performed a clear proof, on their terms, showing that the SARS-CoV-2 virus is harmless to human beings. That is the only possible conclusion, but, unfortunately, this result is not even mentioned in their conclusion.
These study findings may remind readers of WHO’s initial claim that China had no evidence of human-to-human transmission of the ‘virus’, and of course a virus that is not infective to humans could not possibly be transmitted from human to human.
This could well be because the cause of disease labelled ‘Covid-19’ is not a virus at all.
Conclusion
As it is, ‘Covid-19’ has no specific set of symptoms. What began as pneumonia from an unknown cause in 17 patients in Wuhan quickly morphed into a disease with an ever expanding smorgasbord of symptoms, the natural result of relying primarily on flawed PCR testing rather than a specific set of symptoms to diagnose patients. Wuhan has some of the worst air quality in the world, and pneumonia could easily be caused by this toxic environment. Some of the cities with the greatest number of Covid patients also have some of the worst air quality in the world.
There are a great many various potential causes for the myriad of symptoms being falsely attributed to Covid. We should not forget that the mysterious ‘disappearance’ of the flu magically coincided with the emergence of ‘Covid-19’, and could account for hundreds of thousands of so-called Covid patients, as there are typically some 600,000-800,000 flu hospitalizations in the US every year, with the respiratory illness also accounting for 40,000-60,000 deaths annually. A large number of Covid patients have common flu-like symptoms, while a great many also have much milder symptoms resembling the common cold, another coronavirus, the presence of which could easily trigger a positive PCR or antibody test result. Many more never have any symptoms at all.
The evidence that other diseases are being ‘diagnosed’ as ‘Covid-19’ cases is abundant, and has in fact been openly admitted by the very officials we are told to trust. They may have been hospitalized (and in many cases died) due to other causes, but because PCR test results came back positive, they are presumed infected and listed in the official Covid case count. Such is how the Covid illusion is perpetuated, and can be perpetuated into eternity.
As David Crowe writes in his comprehensive paper, “Flaws in Coronavirus Pandemic Theory”:
The world is suffering from a massive delusion based on the belief that a test for RNA is a test for a deadly new virus … If the virus exists, then it should be possible to purify viral particles. From these particles RNA can be extracted and should match the RNA used in this test. Until this is done it is possible that the RNA comes from another source, which could be the cells of the patient, bacteria, fungi, etc. There might be an association with elevated levels of this RNA and illness, but that is not proof that the RNA is from a virus. Without purification and characterization of virus particles, it cannot be accepted that an RNA test is proof that a virus is present.
Definitions of important diseases are surprisingly loose, perhaps embarrassingly so. A couple of symptoms, maybe contact with a previous patient, and a test of unknown accuracy, is all you often need. While the definition of SARS, an earlier coronavirus panic, was self-limiting, the definition of the new coronavirus disease is open-ended, allowing the imaginary epidemic to grow. Putting aside the existence of the virus, if the coronavirus test has a problem with false positives (as all biological tests do) then testing an uninfected population will produce only false-positive tests, and the definition of the disease will allow the epidemic to go on forever.
This strange new disease, officially named COVID-19, has none of its own symptoms. Fever and cough, previously blamed on uncountable viruses and bacteria, as well as environmental contaminants, are most common, as well as abnormal lung images, despite those being found in healthy people.
He then concludes that: “The coronavirus panic is just that, an irrational panic, based on an unproven RNA test, that has never been connected to a virus. And which won’t be connected to a virus unless the virus is purified. Furthermore, even if the test can detect a novel virus the presence of a virus is not proof that it is the cause of the severe symptoms that some people who test positive experience (but not all who test positive).”
Indeed, the available scientific research appears to indicate that this ‘virus’ is in fact not the cause of the symptoms of those who test positive, not even shown to be able to damage human cells in any way at all...
Meanwhile the perpetuation of this Covid illusion into eternity is additionally facilitated by the perpetuation of ‘pandemic’ measures, with lockdowns and isolation weakening the immune system, long term mask use demonstrably capable of leading to bacterial pneumonia, and the injections demonstrably causing Covid-like disease in recipients, with the mechanism by which the jabs could literally be causing ‘Covid-19’ now well established in scientific literature. And so the grand illusion can quite easily be perpetuated indefinitely, so long as the public remains ignorant to the many facets of this illusion and the foundation upon which it has been constructed.
The whole world has been ‘diagnosing’ millions of people almost exclusively with a test designed to detect a theoretical computer-generated virus that has never been proven to exist or to cause disease labelled ‘Covid-19’, and many hundreds of millions of ‘vaccine’ doses formulated to ‘protect’ against the same theoretical virus have been injected into the arms of men, women and children across the planet.
To call this medical fraud would be an understatement. It is a crime against humanity and the crime of a century, being used to enslave the entire human race and usher in the biosecurity state apparatus of an Orwellian technocratic world order. And for the sake of humanity and the freedom of all mankind, it must be immediately stopped in its tracks, before one day it is too late and the world we once knew has faded from our memory completely, replaced by the global prison being built around us, with all those who dared resist the madness destroyed along with all remnants of sanity and freedom.

damn really
Makia Freeman has an account in Steem and thus Hive according to his article here. Yet I was unable to find it by searching. If you know a way of contacting this person please let me know, I'd like to give her (or him) a mention.