
I was on call from the 12th of July to the 19th. I was told that the unit I was in was going to be a chill place and that we hardly have any cases but Paediatric Surgery showed this was not the case. Even though now I am few days from finishing this unit and I realize that what I am complaining about in this week was actually nothing to complain about when compared to the call week I just finished.
I called the chief resident and asked which unit I would be joining and when I was told I would be in pediatric surgery, there was no leaping for joy...It was a sad moment for me because I just finished a posting that other house officers would describe as hard. Having finished that department I was told I was going to be moved to an easier department like orthopedics. So...I was sad but I braced myself for the worse.
I was told that they were in the theatre that Monday, yet another thing I didn't plan for. I hadn't ironed my scrubs and I like to know that the reason I am wearing unironed scrubs is that I was lazy and not because circumstances happened that I couldn't predict.
When I got to the theatre we were handling the hypospadias case. I was also told that we're on call that week. So, everything sad happened to me all at once.
When the call started we had just two patients, one that has urosepsis due to a posterior urethral valve obstruction and a case of hypospadias.
The surgery had just started and I was to give the pre-anesthetic antibiotic.
Source
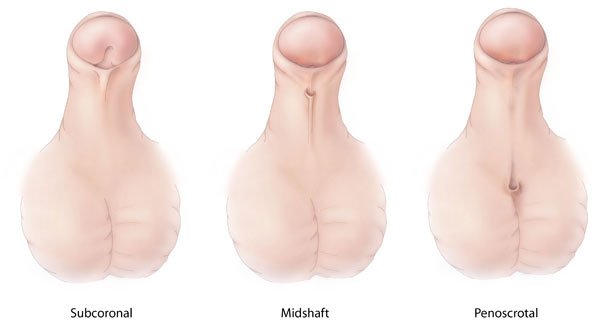
DIFFERENT TYPES OF HYPOSPADIA
Hypospadia
Hypo in greek means beneath and spadia is derived from the Greek word spas meaning torn from and when you put that together...it doesn't even make any sense. But I guess what the greeks were trying to say was that below the penis is torn because that is what hypospadia appears to be, a torn penis.
Hypospadia is a condition where there is an abnormal urethral opening on the penis. Instead of coming out of the tip, it comes out on the shaft, the glans, or in between the shaft and the scrotum.
Based on the position of the opening hypospadias derive their names. It could be glandular hypospadias, coronal hypospadia, a midshaft, or penile hypospadia, it could be penoscrotal hypospadia or a scrotal hypospadia.
It typically happens between the 8th and 14th week of pregnancy this is typically around when sexual differentiation begins to take place in utero. Before that, the genitalia of the male and female fetuses are alike.
When under the influence of testosterone, the male fetus begins to have some more masculine features and then female genitalia is not affected by this hormonal interplay. It does not secrete as much testosterone as the male fetus.
If there is any abnormality in the secretion of the hormones, there could be ambiguity of the genitalia, leading to abnormal genitalia with masculine and feminine features such as clitoromegaly...(an abnormally large clitoris that looks almost like a penis) or micropenis, a small penis that looks like a clitoris.
As the urethra, which is initially like a groove closes to form a hollow opening it migrates to the tip of the phallus...But it may stop along its way to form hypospadias. Read more here and here.
We did a mini ward round after the surgery where I was introduced to the second case by the registrar. This was a case of a Posterior urethral Valve Obstruction.
Source
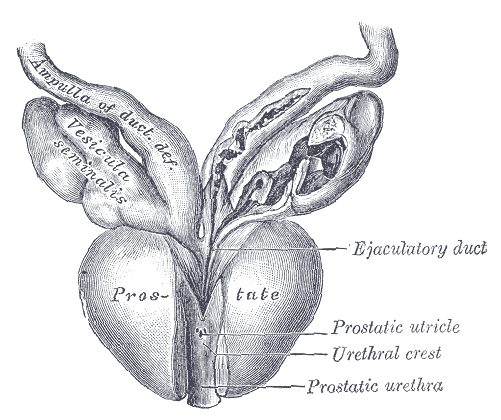
POSTERIOR URETHRAL VALVE BEHIND PROSTATIC URETHRA
Posterior Urethral Valve (PUV)
A posterior urethral valve obstruction is a condition that arises by chance and affects only males. Usually, the fetal tissue that causes the obstructions is not supposed to be there. It can be mild or very severe...so much so that it can cause kidney damage or respiratory failure and ultimately lead to death.
Doctors typically abbreviate it to PUV. When a woman goes for her regular antenatal visits an Ultrasound will show findings of hydronephrosis and in greek, hydro-water, and nephro-kidney together meaning water kidney. The mother usually has features of Oligohydramnios that rise when the normal flow of fluids can not take place in the fetus leading to reduced amniotic fluid (the fluid that bathes the fetus in the womb).
The radiologist will see areas branching out around the kidney that has water in them represented in black (anechoic). The method of diagnosing it when the child is born is typically with a voiding cystourethrogram.
Surgery inutero has a poor outcome with about 43% of cases ending in death. Read the study published on NCBI here
The main method of treatment is valve ablation or in severe cases urinary diversion.
Valve ablation as the name implies is a destruction of the valve. For it to be done, a small telescope device is inserted into the patient's urethra and is used to view this causative valve and with the use of probes that are attached to the telescope, the valve is being removed.
I am yet to find out if this hospital has that type of equipment to do this special telescoping (cystoscopy) but I have seen a laparoscopic surgery (where a small telescope device is used to view the abdomen) being done here.
In a urinary diversion, there is usually a dysfunctional aspect of the urinary tract like in PUV where there is an abnormal tissue blocking the other end of the ureter. In diversion the ureter can be connected directly to the abdominal wall and diverted through that opening or, it could be connected to the bowels (sigmoid colon) or the bowel could be attached to a segment of the bowel and attracted to the skin...there are many procedures for diversion really, but generally speaking urine is just being diverted.
When we were asked to see a patient at the Children's Emergency Room during the call for a case of what we presumed was just appendicitis especially from the general physician's notes they left. The patient had a fever, abdominal pain and had been vomiting. Everything started around the same time. It was a 16-year-old boy and the most had been done to stabilize him before we arrived. He had intravenous access placed on him, he was receiving fluids. He was the first case we saw that was directly related to our call.
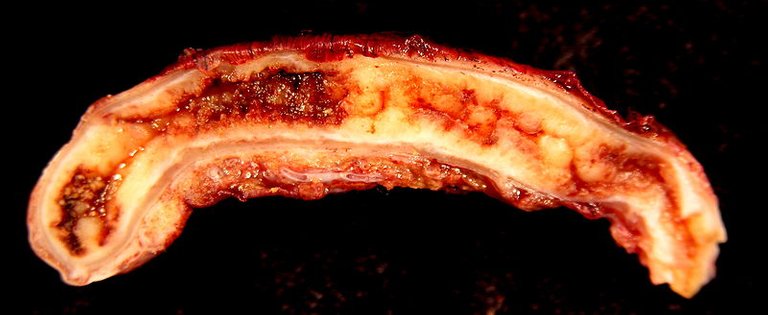
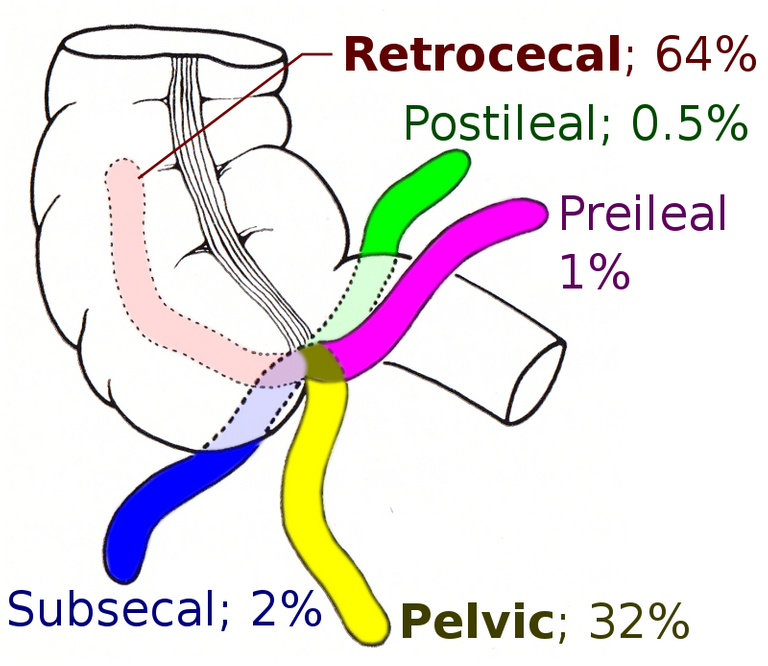
Appendicitis
Appendicitis is an inflammatory condition of the vermiform appendix, a vestigial organ attached to the cecum (bowel).
When We got there he was in painful distress, Crying out in Igbo "ọ na -afụ ụfụ" meaning- it's painful. He didn't speak English.
His caregivers were a group of men, which is usually atypical for pediatric cases. Usually, there are one or two female care giver primarily station to take care of the patient. But in this case, there were just men. I hypothesized that the boy was an apprentice being trained in the art of sales and he developed the abdominal pain for which he was encouraged to deal with until he could no longer function effectively at his work.
His abdominal pain was distinct and was typical of the way appendicitis presents to the hospital. It was a right lower quadrant pain that was sharp. Read more here
He was given intramuscular pentazocine which I got to find is used in older children in this hospital. Studies were done on its effectivity
He was given intravenous fluid for the meantime as we also told him not to eat as he would be going in for surgery as early as possible.
We kept him on intravenous fluids also so that he could be prepared for surgery.
I wrote the Emergency operation list for the team. It usually has the heading, the number of patients to be operated on, the name of the patient, the age, the sex, the folder number of the patient, the ward of the patient, the diagnosis, the procedure to be done don't the patient. The surgical team, the anesthetic team, and the Nurse anesthetic team
I wrote a consultation letter to the anesthetic team to come to see the patient.
If he was going to go for surgery and anesthesia to be used on him, he ought to be on an empty stomach so that he doesn't aspirate fluid to his lungs...basically vomiting into his lungs.
Pre-anesthetic antibiotics were given so that there would be a cover for the bowels before they get exposed and get handled by the surgeon.
The antibiotics that are usually given are Metronidazole and Ceftriaxone. We gave the 500mg of metronidazole and 2g of ceftriaxone...both adult doses because he was a 16-year-old.
A McBurney-McArthurs incision was made at McBurney's point the lateral two-thirds of the imaginary line drawn between the umbilicus and the Anterior Superior Illiac Spine.
The incision was made through the skin, subcutaneous fat, muscle before entering into the abdominal cavity. There was difficulty finding the appendix because the incision was too small, eventually, it had to make wider with blunt dissection with the gloved fingers.
Then when we looked through the bowels we saw the cecum and the appendix was attached to it. We however found that the appendix was necrotic and had pus all over it. After removing the appendix (that basically fell off because it was not receiving blood supply,) the bowel was irrigated with normal saline, and a draining tube was placed to drain the cavity.
The last case that came to the theatre was a similar case to the case I just described.
Appendicular Mass
When we got to the Children's Emergency Room, she was in painful distress and did not want to be examined by my colleague. When he examined her abdomen the 8-year-old had rebound tenderness and central tenderness around the umbilicus which showed that she had peritoneal affectation.
The ultrasound done confirmedwhat the examination had already shown. She also had a history of a formal diagnosis of an appendicular mass from a neighboring hospital. She was asked to come back to the hospital in 3 months but appeared to our Emergency after 6 months.
It is not atypical for patients or their caregivers to think that certain diagnoses will not follow their course. Typically surgery is done after 3 months to take out the mass but the mother didn't take the girl back to the hospital for whatever reason and there she was in our Emergency room with more exaggerated symptoms than she would have if she came 3 months earlier.
she had been stabilized and pain medication given and her surgery was done the day after she presented.
The incision made on her abdomen was a midline incision to expose the whole abdomen so that the cause and effect of the peritonitis could be properly examined.
After all the layers of the abdomen had been exposed to get to the abdominal cavity, we made it to an abdominal cavity that was filled with fluid and would have to be properly irrigated with Normal saline.
After the abdominal mass was found and taken as a sample for the lab scientists at the laboratory to investigate what exactly it was, the abdomen was closed up she was sent to the recovery room where post-operation intravenous antibiotics were given.
I struggled at first to sort out my responsibilities in the ward but eventually, I came to realized that my responsibilities in the theatre triumphed my responsibilities in the ward.
There was a third patient we were asked to see at the Children's Emergency Room with similar features of abdominal pain. The 7-year-old girl's case was a peculiar one. She was not in painful distress and abdominal palpations did not reveal tenderness on the right iliac fossa as was the case of other cases of suspected appendicitis instead she had left iliac pain.
As we soon got to find out she had been to the hospital for these symptoms before and was admitted by the other pediatric surgery team. My hands were already full so I didn't get the full details of the case after we handed it over to the other team but the last I heard was that she was being given oral medication.
Honestly, I had a hard time following the medical jargons, but it was an interesting read. !discovery 35
Ok...thanks for stopping by...I'll try to tone it down next time.
You may continue with how you write your blogs. I looked it up in the net and learned something from reading it. Maybe add some little explanation on the medical jargons. By the way, continue sharing your medical experience. Enjoy some !PIZZA
@ebingo! I sent you a slice of $PIZZA on behalf of @juecoree.
Learn more about $PIZZA Token at hive.pizza (6/10)
Thanks. I'm glad you learnta thing or two.
Thanks for the pizza!
Its an interesting write-up of pediatric surgery that's related to healthcare. I am from not medical background o cant understand but liked it and enhanced my knowledge as well a bit. thanks for sharing
You're welcome....I'm glad you learnt a thing or two
This post was shared and voted inside the discord by the curators team of discovery-it
Join our community! hive-193212
Discovery-it is also a Witness, vote for us here
Delegate to us for passive income. Check our 80% fee-back Program
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider supporting our funding proposal, approving our witness (@stem.witness) or delegating to the @stemsocial account (for some ROI).
Please consider using the STEMsocial app app and including @stemsocial as a beneficiary to get a stronger support.