An ultra far-right, authoritarian homophobe/transphobe will soon assume the presidency of Brazil[1] and according to a memo leaked a couple of weeks ago, the Trump administration is planning to narrow the definition of gender to be immutable and determined at birth[2]. This would in practice eliminate protections at work, school or other settings for trans people and any other individual whose gender differs from the sex they were assigned at birth. The memo claims this would be done because gender needs to be determined "on a biological basis that is clear, grounded in science, objective and administrable.” I have actually had (internet) discussions with people who claim there's no more nuance beyond being born male or female and that science backs their view. I'm not sure which science is this one that denies the existence of people we can empirically observe by the millions.
Given all this, I thought we should actually look at the science so we can make informed decisions on matters that affect people's lives. Approaching LGBT+ issues can be a delicate subject: it can easily trigger those on the right or leave different members of the LGBT+ community feeling misrepresented. My objective here is to reach those who want to learn more about the actual science of human sexual development but also those who may be sitting on the fence or sort of thinking that “maybe these LGBT people are getting out of hand.”
First, let’s set down some terms
- Sex (noun not verb!): A category we use for species that reproduce sexually. Also, for us humans it’s something medical professionals or authorities assign to new-born babies (although this determination can also occur before birth) based on the genitalia observed. Some are not born with traditional male or female genitalia, as is the case of intersex people[3]
- Gender identity: This is how people self-identify. Usually, people identify as what is traditionally understood to be male or female, but others feel differently, such as being agendered or genderfluid, highlighting how this identity can run in a “spectrum[4,5].” Interestingly, some societies have long histories of distinguishing more than two genders[6]
- Sexual orientation: This refers to which sex and gender people find themselves attracted to. Heterosexuality is the most common orientation but I’m sure you have heard of asexuality, homosexuality or bisexuality, also highlighting how this orientation can run in a non-binary “spectrum”
- Gender expression: This is how a person behaves and looks and how their society perceives that look and behaviour
- Gender dysphoria: Refers to the distress that arises when individuals face incongruity between their assigned sex at birth and their internal experience of gender[7]. This feeling usually begins in childhood and can oftentimes disappear after puberty. Most, but not all, transgender people experience it.
There are even more ways in which people identify their gender identity or sexual orientation than the ones mentioned above and as best as our science goes this is not a conscious choice[8,9] (and even if it was, it wouldn't be anybody else’s business, would it?) but something determined largely or completely by your biology, something that you feel deep inside. If, for example, you are a straight male who feels at home in a male body and feels attraction to females, then you know how deep those feelings are and how inherent to who you are. In part 2 we will look at some aspects of the neurobiology of sex and gender, which should help you find an indication of where these feelings come from.
Describing feelings can be difficult so it’s no wonder different people come up with different labels for who they are and why the terms you may be familiar with do not apply to them. Furthermore, we are talking about the intersection between physical sex, gender identity (and expression) and sexual orientation which can all be non-binary and also move independently from each other at least to some extent[4]. This creates a rather big canvas of possibilities, which, again, explains why the traditional male and female labels do not apply to any number of individuals you may meet in the real world. So maybe next time you should stop to think before you start talking about “attack helicopters.”
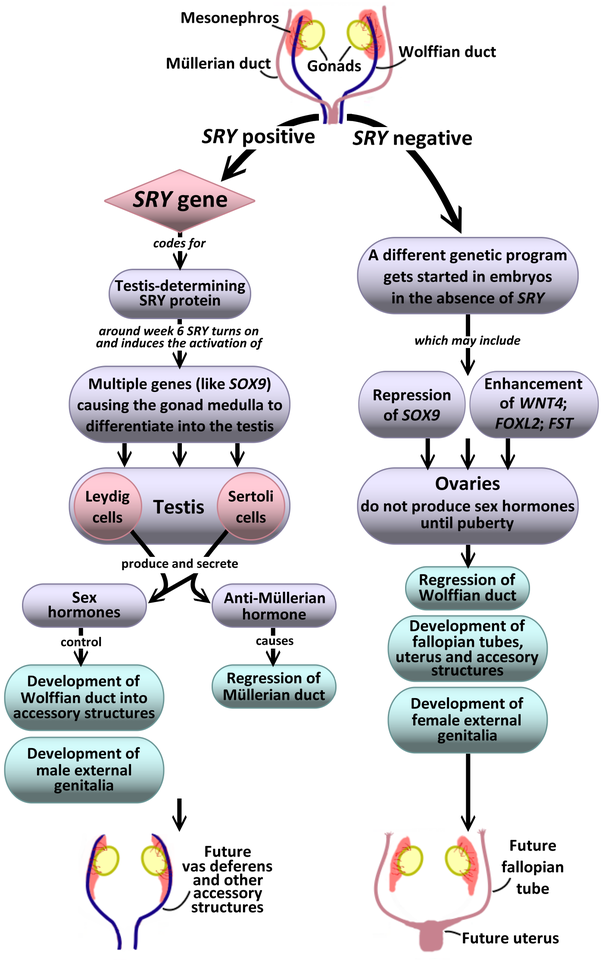
Figure 1. Schematic representation of the internal sexual structures in humans before and after the masculinization or feminization genetic programs are initiated. We are covering a period here that goes from around week 6 to around week 12 of development. Adapted from public domain source by Dee Silverthorn and a paper by SG. Tevosian[21]
How does sex determination work?
You probably know the human genome is organized into 23 pairs of chromosomes, one set of 23 is inherited from the mother and the other from the father. The “sex chromosomes" make one such pair and are so named, in an undoubted bout of originality, because they are essential in determining the sex of the individual. The chromosomes in the other 22 pairs are called “autosomes” and they also play a role in sexual development. Some people love to point out that “XX=female and XY=male and that’s it!” but the reality is more complicated. Our brain loves to put things into neat categories, yet nature is far too complicated for neat categories.
With that in mind, we can focus on the Y chromosome, which carries a master gene for sex determination known as “SRY.” Initially, XX and XY embryos don’t really seem to differ, it’s only after the SRY gene is activated that those who carry it start developing testicles (see Figure 1). You could say that the “default” developmental pathway is that of developing ovaries.
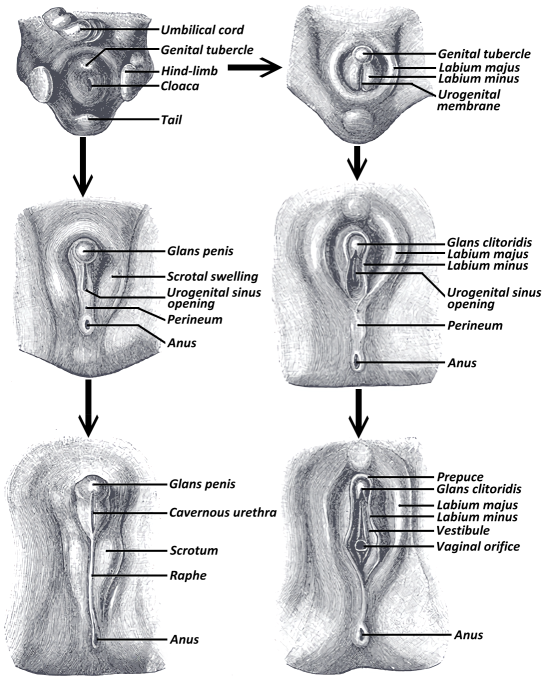
As the testis develop, they start producing and secreting sex hormones (primarily androgens like testosterone, although estrogens are also produced and needed for normal sexual function and development), which go on to further masculinize the body. Most of the sexual structures have a common point of origin between the two sexes. For example, the primordial gonads can become testis or ovaries while the clitoris and the glans derive from the same precursor, as do the scrotum and outer labia (see Figure 2 below).
But nature doesn’t do categories:
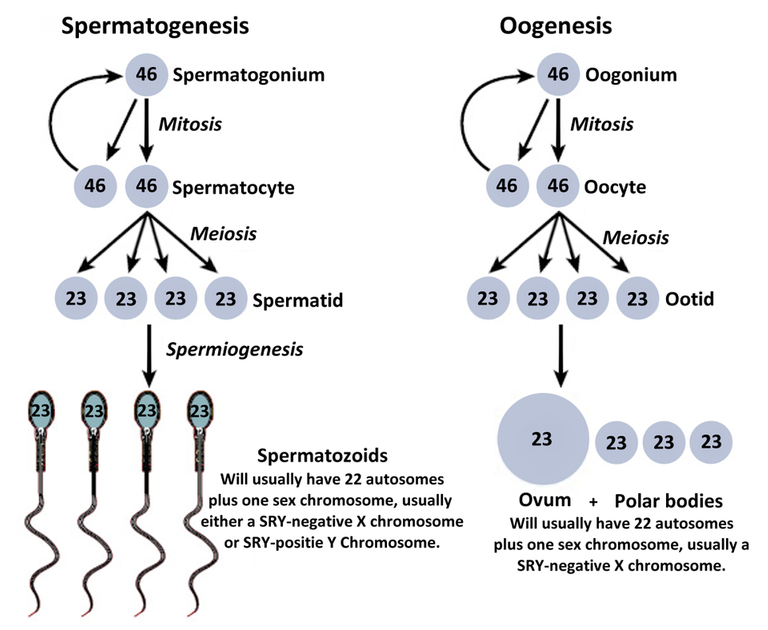
Figure 3. Schematic representation of gametogenesis for sperm (left side) and eggs (right side) in humans. The numbers inside the cells represent the number of chromosomes. Mitosis basically creates clones of the original cell, useful for growth or replenishment. Notice how cells don't change their number of chromosomes after mitosis. Meiosis specifically creates gametes. Each pair of chromosomes interchange genetic material with each other (a process known as "genetic recombination") and the daughter cells typically end up with half the chromosomes as they will join another gamete to create an embryo with 46 chromosomes. Cell sizes are not to scale. Adapted from CC BY 3.0 source by OpenStax College.
- Sometimes during gametogenesis (the process that gives rise to sperm or egg cells, see Figure 3 to the right) the SRY gene can be copied into an X chromosome and/or be excised from the Y chromosome meaning some people can be XX SRY-positive[10] or XY SRY-negative[11]
- Other times, different numbers of sex chromosomes can hitch a ride into a gamete leading to people who can be XXX, XXY or XXXY among other clinically described possibilities[12]
- Yet other times, people may carry XY SRY-positive sex chromosomes plus androgen receptors that respond differently from what’s typical[13].
This is an incomplete list but we already have numerous examples of people who behave and look typically “male” or “female” but do not conform to the “XX=female and XY=male and that’s it!” narrative. In other cases, we're talking about different kinds of intersex people who can have genitals/gonads that don’t conform to traditional “male” or “female” categorization. There can even be variability within a particular group, both in terms of physical sexual characteristics and personal identification. For example, XX intersex individuals can present different physical sexual attributes and may choose treatment to further their primary and secondary sexual characteristics into the typical male or female form[14]. This can happen because, as we review in part 2, the degree of masculinization/feminization of the sex organs can differ from the degree of masculinization/feminization of the brain[15].
Until very recently, it was still common for doctors to look at the genitalia of an intersex baby and perform surgery to remove whichever parts they thought best, thus assigning a sex of their choice to the new-born. Can you imagine self-identifying as a male but being brought up as a girl and later learn that some doctor operated on your genitals to make them conform to a more typically female form at the moment of your birth? Or vice versa? While there's a long way still to go, intersex individuals have been gaining more understanding and rights recently. Non-consensual and irreversible surgery (which can include forced sterilization) of infants has been severely criticized with different levels of accompanying legal reforms in jurisdictions such as Australia (in 2013)[3], Europe (2015)[3,16] or Chile (2016)[17].
To finalize this section I would like to mention another group of intersex people who are XY SRY-positive and have reduced expression of one particular sex hormone. They can be born looking fully female externally, grow up to usually identify as male and once puberty strikes go through masculinization, up to and including growing a penis[18,19,20]. So as you can see, nature really doesn’t do categories.
Hopefully, some of you are starting to see that claims like “there are only two sexes” are too simplistic compared to the variety of situations that can actually occur naturally. To rely on the decision that somebody else made for you at the moment of your birth, and perhaps make it legally immutable, is an affront to your personal freedom and dignity, to your basic human rights.
You can now continue on to part 2, where we review what we know about the feminization/masculinization of the brain, transgender people and hopefully convince you that we shouldn't make life more difficult than it needs to be for each other.
Notes:
After making this post, I learned of a statement published on October 26th signed by more than 700 biologists, over 100 geneticists, and nine Nobel Prize winners (it's currently signed by more than 2600 scientists) condemning the leaked proposal by the Trump administration to change the definition of gender. You can read the statement here and a news article here.
References:
[1] "The lessons for western democracies from the stunning victory of Brazil’s Jair Bolsonaro" published by The Intercept
[2] "‘Transgender’ could be defined out of existence under Trump administration" published by The New York Times
[3] "Intersex - Fact sheet" published by United Nations Free & Equal
[4] Transgender and gender nonconforming adolescent care: psychosocial and medical considerations (2015) Curr Opin Pediatr. 27(4):421-6
[5] Gender identity development in adolescence (2013) Horm Behav. 64(2):288-97
[6] "Third gender" article at Wikipedia
[7] Research priorities for gender nonconforming/transgender youth: gender identity development and biopsychosocial outcomes (2016) Curr Opin Endocrinol Diabetes Obes. 23(2):172-9
[8] Evidence supporting the biological nature of gender identity (2015) Endocr Pract. 21(2):199-204
[9] Approach to the patient: transgender youth: endocrine considerations (2014) J Clin Endocrinol Metab. 99(12):4379-89
[10] 46 XX karyotype during male fertility evaluation; case series and literature review (2017) Asian J Androl. 19(2):168-172
[11] Clinical and pathologic spectrum of 46,XY gonadal dysgenesis: its relevance to the understanding of sex differentiation (1991) Medicine (Baltimore). 70(6):375-83
[12] Sex chromosome aneuploidies (2018) Handb Clin Neurol. 147:355-376
[13] Androgen resistance (2006) Best Pract Res Clin Endocrinol Metab. 20(4):577-98
[14] Consensus statement on management of intersex disorders. International Consensus Conference on Intersex (2006) Pediatrics. 118(2):e488-500
[15] Sexual differentiation of the human brain: relation to gender identity, sexual orientation and neuropsychiatric disorders (2011) Front Neuroendocrinol. 32(2):214-26
[16] "Human rights and intersex people" published by the Council of Europe
[17] "Chilean goverment stops the 'normalization' of intersex children" published by OutRight Action International
[18] Androgens and the evolution of male-gender identity among male pseudohermaphrodites with 5alpha-reductase deficiency (1979) N Engl J Med. 300(22):1233-7
[19] Gender change in 46,XY persons with 5alpha-reductase-2 deficiency and 17beta-hydroxysteroid dehydrogenase-3 deficiency (2005) Arch Sex Behav. 34(4):399-410
[20] "The extraordinary case of the Guevedoces" published by BBC Magazine
[21] Genetic control of ovarian development (2013) Sex Dev. 7(1-3):33-45
As a follower of @followforupvotes this post has been randomly selected and upvoted! Enjoy your upvote and have a great day!
This was a phenomenal post! Thank you for working through a (non-exhaustive) list of various genetic combinations and some of their effects. Resteemed!
Let me make sure I'm understanding: the SRY gene is normally associated with the Y chromosome, right? But SRY is not always present even on Y chromosomes?
Finally, of course, no doctors are doing complex genetic testing at birth, so they're just doing a quick visual inspection and assigning sex at birth. Hence, much room for overly-simplified error?
Thanks! Sorry if it wasn't too clear, Y chromosomes usually have the SRY gene but sometimes they don't (and there are other genes involved too, but SRY seems to be the important one that sets things in motion)
And yes basically the doctor looks at the genitalia and that's it. I think nowadays some things are normally tested (like XXY or XXX) but I'm not an expert, I don't know which genetic or chromosomal tests are common nowadays.