The third lecture of the PrEParing course second week is “Emerging Data/Ongoing Trials for PrEP,” introduced by Neha Pandit, Associate Professor of Practical Pharmacology at the School of Pharmacy at the University of Maryland (USA).
There are three categories currently investigational products for HIV pre-exposure prophylaxis are broken down into three categories:
- Which have already been approved for use as part of antiretroviral therapy;
- New antiretroviral drugs;
- Already approved as another class of medicines;
Also, scientists are trying to develop various modalities for how these drugs are administered including vaginal and rectal rings, gels, self-dissolving films, long-acting soft implants, solutions for the rectal douche.
The only drug that has already been approved by the US Food and Drug Administration (FDA) for PrEP is Truvada — a combination of tenofovir disoproxil fumarate and emtricitabine. Let’s consider the molecules with which researchers connect the future of PrEP.
TAF
Tenofovir disoproxil fumarate or TDF is a prodrug for TFV which is tenofovir. TDF requires a transformation so that the medicine begins to work.

Figure 1 — TDF and TAF pharmacokinetics in blood plasma and inside the lymphocyte. Source: Mills A, et al. J Acquir Immune Defic Syndr 2015; 69(4):439-45.
What you can see from Figure 1 is that TDF is transformed to tenofovir in the plasma and then also transformed to more tenofovir inside the lymphocyte. TAF, or tenofovir alafenamide, has lower levels of tenofovir in the plasma but achieves a higher concentration of tenofovir in the lymphocyte or where the side of action is.
It turns out that TAF blocks HIV while its blood plasma levels much lower than TDF, which means less toxicity for the liver and kidneys. Researchers aspire to use this TAF feature to develop a drug for PrEP with minimal toxicity. One of the factors to take into consideration is the concentration of both of these medications in mucosal tissue of the mouth, genitals, and rectum where the drug reliably protects the body against HIV exposure.
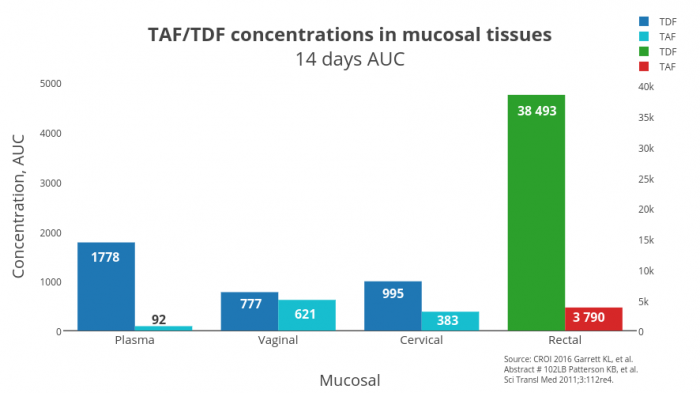
Figure 2 — Concentration distribution for TDF and TAF in the mucosal tissues of the vagina, cervix and rectum. Source: CROI 2016 Garrett KL, et al. Abstract 102LB Patterson KB, et al. Sci Transl Med 2011;3:112re4.
So we know that TAF achieves higher concentration within the cell than TDF does. But what happens in mucosal tissues? Take a look at the chart (Figure 2) — the concentration of TAF in the mucous membranes of the vagina, cervix, and rectum is lower than TDF. Rectum levels are of red and green color since TDF reaches high concentrations in this tissue.
Hence TDF is better than TAF reaches high levels in mucosal tissues and is probably better suited for PrEP, although TAF is much less toxic.
But researchers don’t give up, conducting a study for TAF as PrEP on twelve monkeys, six of which receive PrEP as a combination of TAF and emtricitabine (FTC), and the other six do not receive PrEP. These monkeys are periodically injected into the rectum with a solution of the simian/human immunodeficiency virus (SHIV).
The result is striking — none of those primates that were treated with PrEP actually caught the virus, while six individuals who did not receive PrEP became SHIV-positive. The researchers went further and turned to the third phase of a clinical trial recruiting transgender women and men who have sex with men (MSM).
Maraviroc
Last year, a report on the second phase of the clinical trial of Maraviroc for PrEP was published. The investigators tested Maraviroc on 406 men who have sex with men (MSM). Impressive results are already available — five of the subjects caught HIV. Four of them are likely due to noncompliance whereas the one who was compliant to the medication though develop HIV did not have any resistance to maraviroc.
Another study of Maraviroc as PrEP was done in 188 females Maraviroc, not a single case of HIV transmission was reported.
The Pharmacokinetics of Maraviroc shows a decreased mucosal tissue concentrations, perhaps a combination with another substance will block HIV better, similar to how tenofovir and emtricitabine are given.
Cabotegravir
The study of cabotegravir for PrEP conducted ingeniously:
- first, participants were prescribed 30 mg of cabotegravir once a day orally (tablets) for four weeks;
- next, they were provided with injections of 800 mg of Cabotegravir intramuscularly every 12 weeks, for three doses.
127 of the low-risk group were involved in the study where 106 of them were prescribed cabotegravir as PrEP. Transmission of HIV occurred only in one participant. After the study, the subjects were asked to answer the question:
“Which method would they prefer to receive PrEP: as a daily tablet or injection every 12 weeks?”
62% of the subjects would prefer injections, 23% reported that both methods of PrEP are equally convenient.
Dapivirine
Dapivirine is a new non-nucleoside reverse transcriptase inhibitor, approved recently by FDA for HIV treatment. For PrEP it comes as a vaginal ring with 25 mg of dapivirine inserted monthly.
The concentrations of Dapivirine achieve its effective level 8 hours after insertion into vagina. This advantage over oral PrEP medications, which are able to reach sufficient levels in mucosal tissues after 2-7 days. Besides, the ring forms a locus of a high HIV-blocking substance concentration in mucosal tissues of the vagina, without exposing internal organs to toxic effects.
Two coextending clinical trials were conducted for the study of dapivirine as PrEP. The most comprehensive of them involved 2,629 African-American women. Half of them were offered to use vaginal rings with dapivirine, the other half prescribed vaginal rings with a placebo (without dapivirine).
Finally, researchers reported 168 cases of HIV transmission, where 71 of them were in the dapivirine group, and 97 cases in the placebo group. The reduction in the risk of HIV transmission among women prescribed vaginal rings with dapivirine was 27%.
In the study report, an interesting finding was described — almost all women whose PrEP was ineffective were younger than 21 years. Researchers suggest several reasons for the difference in age groups:
Models of sexual behavior;
- Frequency of sexual acts;
- Number of sexual partners;
- Age of sexual partners;
- Vaginal microbiome structure.
- So understanding why that may have been would be important moving forward.
VRCO1
VRCO1 is a neutralizing monoclonal antibody examined to be given as an infusion every two months for PrEP. Neutralizing monoclonal antibodies help the HIV glycoprotein gp120 not binding to CD4-lymphocytes “chemokine” receptors. As a result, the virus loses its ability to bind with the lymphocyte, so HIV reproduction ceases. Similar techniques are explored for the treatment of cancer, diabetes, hereditary diseases.
VRCO1 is currently being studied as PrEP in the MSM population and the women population. It is assumed that this method of PrEP will be more expensive and provided for people in high-risk groups who may not be able to take an oral medication on a daily basis.
EFdA / MK-8591
EFdA / MK-8591 is a nucleoside reverse transcriptase inhibitor similar to tenofovir or emtricitabine. The new molecule EFdA / MK-8591 is attractive in virtue of a long half-life so it can potentially be given as PrEP in the form of a tablet every six months or even longer.
The lesson is coming to an end. Now many new drugs are being studied for pre-exposure prophylaxis with the aim to help overcome non-compliance issues that we see with tenofovir and emtricitabine and to advance tolerability. Medicines for PrEP could potentially be given every 12 weeks or even annually.
So, Dr. Neha Pandit finished her lecture, and we are waiting for you tomorrow at the lesson “Community-Based Implementation of CDC PrEP Guidelines,” which will be presented by Pierre-Cedric Crouch, the Director of Nursing at Strut San-Francisco AIDS Foundation.
If you have not already signed up for the PrEParing course on the Coursera platform — it’s never too late. Just go to https://www.coursera.org/learn/prep
P. S. The original article was posted on the Life4me+ mobile app for HIV-positive persons blog.