Hello, dear reader. Welcome back to my anatomy series on the upper limb. Today, I want to discuss with you one of the most interesting joints found in the upper limb: the shoulder joint. We'll look at why the shoulder joint is so important and how it works. Other features related to this topic will be addressed as we delve deeper into the article. In case you missed the last topic Scapula, kindly hit the link to review the article.
Why the Shoulder Joint Is Important

The shoulder joint is the most mobile joint in your body. It allows you to move your arm in almost any direction, thanks to its unique structure and the muscles that surround it. The shoulder joint is actually composed of four smaller joints: the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, and the scapulothoracic joint. Together, these joints form a complex system that connects your arm to your torso and enables a wide range of motion.
The shoulder joint is also important for your stability and balance. The shoulder joint helps you maintain your posture and keep your center of gravity. It also helps you transfer force from your legs to your arms, such as when you run, jump, or push something. The shoulder joint is also involved in many sports and recreational activities, such as swimming, tennis, golf, and baseball. Without a healthy and functional shoulder joint, you would have a hard time performing these activities and enjoying life.
How the Shoulder Joint Works
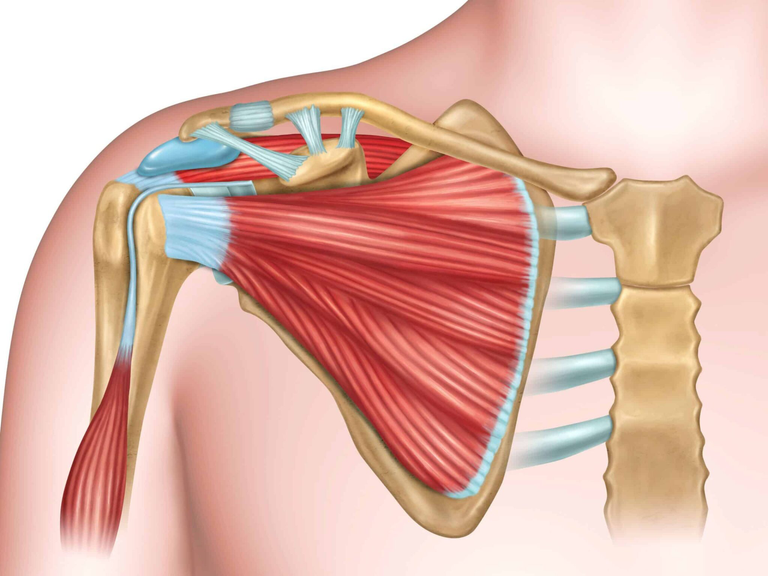
The shoulder joint works by coordinating the movements of the bones, ligaments, tendons, and muscles that make up the joint. The main bone of the shoulder joint is the humerus, or the upper arm bone. The humerus fits into a shallow socket called the glenoid, which is part of the scapula, or the shoulder blade. The glenoid is surrounded by a ring of cartilage called the labrum, which deepens the socket and helps stabilize the joint. The joint is also reinforced by several ligaments, which are bands of connective tissue that connect bones to bones. The most important ligament of the shoulder joint is the coracohumeral ligament, which runs from the coracoid process of the scapula to the humerus and prevents excessive downward movement of the arm.
The shoulder joint also depends on the muscles and tendons that attach to the bones and move the joint. The most important muscles of the shoulder joint are the rotator cuff muscles, which are four small muscles that originate from the scapula and attach to the humerus. The rotator cuff muscles are the supraspinatus, the infraspinatus, the teres minor, and the subscapularis. These muscles help rotate the arm and stabilize the joint. The tendons of the rotator cuff muscles form a cuff around the head of the humerus and blend with the joint capsule, which is a thin layer of tissue that surrounds the joint and contains synovial fluid, which lubricates the joint and reduces friction.
The shoulder joint also works with other muscles that are not part of the joint itself, but help move the arm and the scapula. These muscles include the deltoid, the pectoralis major, the latissimus dorsi, the trapezius, and the serratus anterior. These muscles help lift, lower, extend, flex, abduct, adduct, and internally and externally rotate the arm. They also help move the scapula along the rib cage, which is necessary for the full range of motion of the shoulder joint.
Basic Structure of the Shoulder Joint
Now, we will explore the basic structure of the shoulder joint and learn about its components and functions.
Types of Joint
The shoulder joint is actually composed of four smaller joints: the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, and the scapulothoracic joint. However, the main joint that we will focus on is the glenohumeral joint, which is also called the shoulder joint.
The glenohumeral joint is a synovial ball and socket joint, which means it has a fluid-filled cavity and allows a wide range of motion. It is formed by the articulation between the head of the humerus (the ball) and the glenoid cavity of the scapula (the socket).
Articular Surfaces
The articular surfaces are the parts of the bones that come in contact with each other in the joint. They are covered with a thin layer of smooth cartilage, which reduces friction and protects the bones from wear and tear.
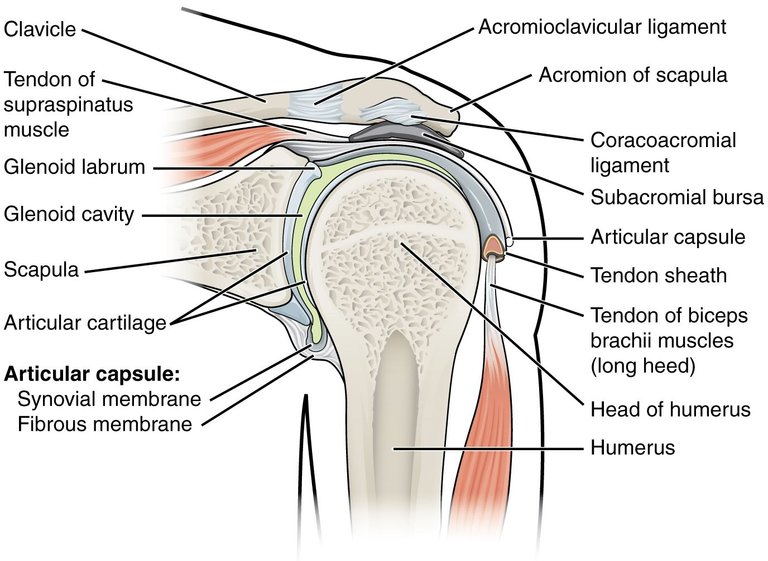
The glenoid cavity of the scapula is a shallow pear-shaped pit on the lateral aspect of the scapula. It is slightly concave and faces laterally, anteriorly, and superiorly. The head of the humerus is a spherical structure that projects from the upper end of the humerus. It is convex and faces medially, posteriorly, and inferiorly.
The head of the humerus is much larger than the glenoid cavity, which means that the joint is not very stable and relies on other structures for support. To increase the congruency of the joint, the glenoid cavity is deepened by a fibrocartilage ring called the glenoid labrum, which attaches to the rim of the cavity and extends beyond it.
Cartilages
Cartilages are flexible connective tissues that provide cushioning and support to the joints. There are two types of cartilages in the shoulder joint: articular cartilage and fibrocartilage.
Articular cartilage is the type of cartilage that covers the articular surfaces of the bones. It is made of hyaline cartilage, which is smooth and translucent. It has a high water content and a low blood supply, which makes it resilient and resistant to compression. It also contains collagen fibers, which provide strength and elasticity.
Fibrocartilage is the type of cartilage that forms the glenoid labrum. It is made of dense connective tissue, which is tough and fibrous. It has a low water content and a high blood supply, which makes it durable and resistant to tension. It also contains elastic fibers, which provide flexibility and shock absorption.
Capsules
Capsules are fibrous sacs that enclose the joints and contain synovial fluid. Synovial fluid is a viscous fluid that lubricates the joint and nourishes the articular cartilage.
The glenohumeral capsule is the capsule that surrounds the glenohumeral joint. It is attached to the anatomical neck of the humerus and the rim of the glenoid cavity. It is thin and loose, which allows the joint to have a large range of motion. However, it also makes the joint vulnerable to dislocation and injury.
The synovial membrane is the inner layer of the capsule that produces and secretes synovial fluid. It is highly vascular and innervated, which means it has a lot of blood vessels and nerves. It also has synovial folds, which are projections of the membrane that extend into the joint cavity and increase the surface area for fluid production.
Ligaments
Ligaments are bands of connective tissue that connect bones to bones and stabilize the joints. They are composed of collagen fibers, which are strong and flexible. They also have some elastic fibers, which allow them to stretch and recoil.
There are several ligaments that reinforce the glenohumeral capsule and prevent excessive movement of the joint. They are:
- The glenohumeral ligaments (superior, middle, and inferior), which extend from the humerus to the glenoid cavity and stabilize the anterior aspect of the joint.
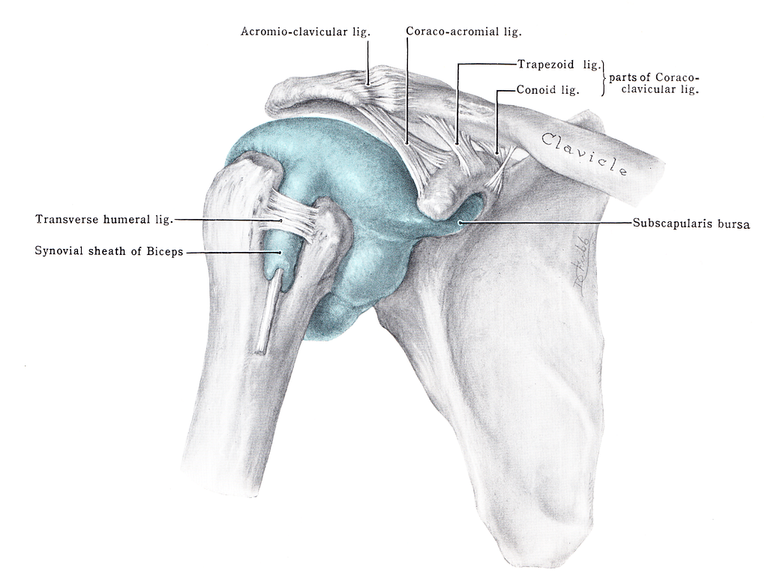
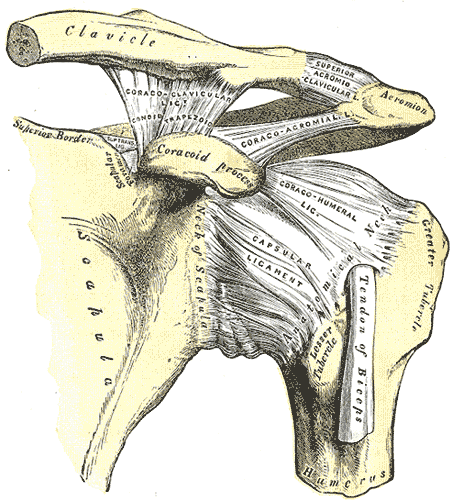
- The coracohumeral ligament, which extends from the base of the coracoid process of the scapula to the greater tubercle of the humerus and supports the superior part of the joint capsule.
- The transverse humeral ligament, which extends between the two tubercles of the humerus and holds the tendon of the long head of the biceps in the intertubercular groove.
- The coracoacromial ligament, which extends between the acromion and coracoid process of the scapula and forms an arch-like structure over the shoulder joint (coracoacromial arch). This resists superior displacement of the humeral head.
Relations
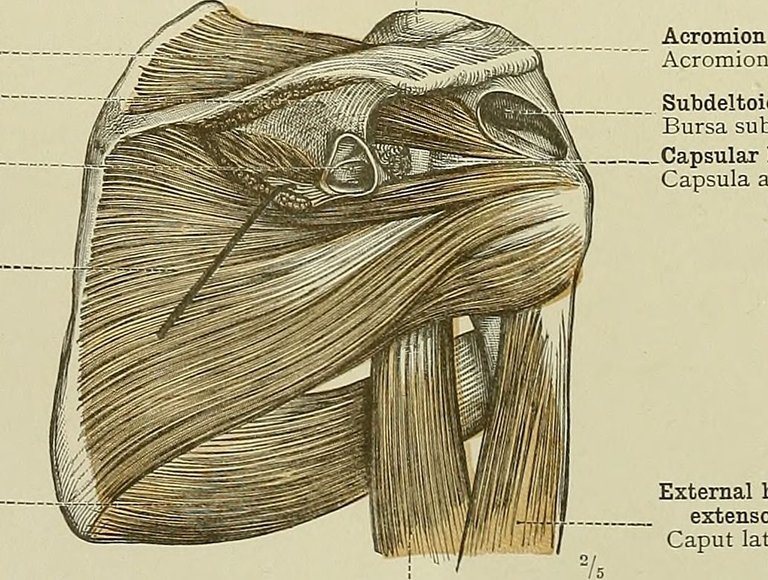
- The rotator cuff muscles, which are four small muscles that originate from the scapula and attach to the humerus. They help rotate the arm and stabilize the joint. They are:
- The supraspinatus, which abducts the arm and assists the deltoid.
- The infraspinatus, which externally rotates the arm and assists the teres minor.
- The teres minor, which externally rotates the arm and assists the infraspinatus.
- The subscapularis, which internally rotates the arm and assists the pectoralis major.
- The biceps brachii, which has two heads that originate from the scapula and attach to the radius. It flexes the elbow and supinates the forearm. The long head of the biceps also crosses the shoulder joint and helps flex and stabilize the joint.
- The triceps brachii, which has three heads that originate from the scapula and the humerus and attach to the ulna. It extends the elbow and assists in extending and adducting the shoulder joint.
- The deltoid, which has three parts that originate from the clavicle, acromion, and spine of the scapula and attach to the deltoid tuberosity of the humerus. It abducts, flexes, extends, and rotates the shoulder joint.
- The pectoralis major, which has two heads that originate from the clavicle, sternum, and ribs and attach to the intertubercular groove of the humerus. It flexes, adducts, and internally rotates the shoulder joint.
- The latissimus dorsi, which originates from the lower back and iliac crest and attaches to the intertubercular groove of the humerus. It extends, adducts, and internally rotates the shoulder joint.
The shoulder joint is also related to several blood vessels and nerves that supply the joint and the surrounding structures. They are:
- The anterior and posterior circumflex humeral arteries, which branch from the axillary artery and encircle the humerus. They supply blood to the joint capsule, the humeral head, and the deltoid muscle.
- The circumflex scapular artery, which branches from the subscapular artery and supplies blood to the scapula and the rotator cuff muscles.
- The suprascapular artery, which branches from the thyrocervical trunk and supplies blood to the scapula and the rotator cuff muscles.
- The subscapular nerve, which innervates the joint itself and the subscapularis muscle.
- The suprascapular nerve, which innervates the joint capsule and the supraspinatus and infraspinatus muscles.
- The axillary nerve, which innervates the joint capsule and the deltoid and teres minor muscles.
- The lateral pectoral nerve, which innervates the joint capsule and the pectoralis major muscle.
Range of Motion and Function of the Shoulder Joint
The shoulder joint is the most mobile joint in the human body. It allows the upper limb to perform a wide range of movements, such as flexion, extension, abduction, adduction, internal and external rotation, and circumduction. These movements are essential for many daily activities, such as reaching, lifting, throwing, and carrying. In this article, we will explore the range of motion and function of the shoulder joint and learn about the factors that affect them.
Flexion and Extension
Flexion and extension are movements that occur in the sagittal plane, which divides the body into right and left halves. Flexion is the movement of the arm forward and upward, while extension is the movement of the arm backward and downward.
The normal range of motion for flexion is about 180 degrees, and for extension is about 60 degrees.
However, these values may vary depending on the individual's age, gender, and physical condition.
The main muscles that produce flexion are the anterior deltoid, the pectoralis major, the biceps brachii, and the coracobrachialis. The main muscles that produce extension are the posterior deltoid, the latissimus dorsi, the teres major, and the triceps brachii.
Abduction and Adduction
Abduction and adduction are movements that occur in the coronal plane, which divides the body into front and back halves. Abduction is the movement of the arm away from the midline of the body, while adduction is the movement of the arm toward the midline of the body.
The normal range of motion for abduction is about 180 degrees, and for adduction is about 45 degrees. However, these values may vary depending on the individual's age, gender, and physical condition.
The main muscle that produces abduction is the middle deltoid, assisted by the supraspinatus. The main muscles that produce adduction are the pectoralis major, the latissimus dorsi, the teres major, and the coracobrachialis.
Internal and External Rotation
Internal and external rotation are movements that occur in the transverse plane, which divides the body into upper and lower halves. Internal rotation is the movement of the arm toward the anterior aspect of the body, while external rotation is the movement of the arm toward the posterior aspect of the body.
The normal range of motion for internal rotation is about 70 degrees, and for external rotation is about 90 degrees. However, these values may vary depending on the individual's age, gender, and physical condition.
The main muscles that produce internal rotation are the subscapularis, the pectoralis major, the latissimus dorsi, and the teres major. The main muscles that produce external rotation are the infraspinatus, the teres minor, and the posterior deltoid.
Circumduction
Circumduction is a complex movement that combines flexion, extension, abduction, and adduction. It is the movement of the arm in a circular or conical pattern around the shoulder joint.
The normal range of motion for circumduction is not well defined, as it depends on the combination of the other movements. However, it is generally limited by the joint capsule, the ligaments, and the surrounding muscles.
The muscles that produce circumduction are the same as those that produce the other movements, depending on the direction and phase of the movement.
Vascular Supply and Nerve Innervation of the Shoulder Joint
The shoulder joint is a highly vascularized and innervated structure. It receives blood supply from several branches of the subclavian and axillary arteries, and nerve supply from the brachial plexus and its branches. In this article, we will explore the vascular supply and nerve innervation of the shoulder joint and learn about their clinical significance.
Vascular Supply
The main arteries that supply the shoulder joint are:
- The suprascapular artery, which branches from the thyrocervical trunk of the subclavian artery. It passes through the suprascapular notch of the scapula and supplies the scapula and the rotator cuff muscles.
- The circumflex scapular artery, which branches from the subscapular artery of the axillary artery. It passes through the triangular space of the scapula and supplies the scapula and the rotator cuff muscles.
- The anterior and posterior circumflex humeral arteries, which branch from the axillary artery. They encircle the humerus and supply the joint capsule, the humeral head, and the deltoid muscle.
The veins that drain the shoulder joint are the corresponding veins of the arteries, which form a periscapular venous plexus and drain into the axillary vein.
Nerve Supply
The main nerves that supply the shoulder joint are:
- The subscapular nerve, which branches from the posterior cord of the brachial plexus. It innervates the joint itself and the subscapularis muscle.
- The suprascapular nerve, which branches from the upper trunk of the brachial plexus. It passes through the suprascapular notch of the scapula and innervates the joint capsule and the supraspinatus and infraspinatus muscles.
- The axillary nerve, which branches from the posterior cord of the brachial plexus. It passes through the quadrangular space of the scapula and innervates the joint capsule and the deltoid and teres minor muscles.
- The lateral pectoral nerve, which branches from the lateral cord of the brachial plexus. It innervates the joint capsule and the pectoralis major muscle.
Stability and Clinical Anatomy of the Shoulder Joint
The shoulder joint is one of the most mobile and versatile joints in the human body. However, this mobility comes at the cost of stability, making the shoulder joint prone to various injuries and conditions. In this article, we will explore the factors that contribute to the stability and instability of the shoulder joint, and the common clinical problems that affect it.
Shoulder Stability
The shoulder joint is a synovial ball and socket joint, formed by the articulation between the head of the humerus and the glenoid cavity of the scapula. The joint is stabilized by a combination of static and dynamic factors, which balance the mobility and stability of the joint.
Importance of Rotator Cuff Muscles
The rotator cuff muscles are four small muscles that originate from the scapula and attach to the humerus. They are the supraspinatus, the infraspinatus, the teres minor, and the subscapularis. These muscles have two main functions:
- They help rotate the arm and stabilize the joint. They act as agonists or antagonists to each other, depending on the direction of rotation. For example, the infraspinatus and the teres minor externally rotate the arm, while the subscapularis internally rotates the arm.
- They compress the humeral head against the glenoid cavity, creating a concavity-compression effect. This increases the stability of the joint by increasing the contact area and the friction between the articular surfaces.
The rotator cuff muscles are essential for the normal function and stability of the shoulder joint. They also form a protective cuff around the joint, preventing excessive displacement of the humeral head.
Role of Ligaments and Tendons in Stability
The ligaments and tendons of the shoulder joint are bands of connective tissue that connect bones to bones and muscles to bones, respectively. They also play a role in stabilizing the joint by limiting the range of motion and reinforcing the joint capsule.
The main ligaments and tendons of the shoulder joint are:
- The glenohumeral ligaments (superior, middle, and inferior), which extend from the humerus to the glenoid cavity and stabilize the anterior aspect of the joint.
- The coracohumeral ligament, which extends from the base of the coracoid process of the scapula to the greater tubercle of the humerus and supports the superior part of the joint capsule.
- The transverse humeral ligament, which extends between the two tubercles of the humerus and holds the tendon of the long head of the biceps in the intertubercular groove.
- The coracoacromial ligament, which extends between the acromion and coracoid process of the scapula and forms an arch-like structure over the shoulder joint (coracoacromial arch). This resists superior displacement of the humeral head.
- The glenoid labrum, which is a fibrocartilage ring that deepens the glenoid cavity and increases the stability of the joint. It also anchors the glenohumeral ligaments and the tendon of the long head of the biceps.
- The rotator cuff tendons, which are the tendons of the rotator cuff muscles. They blend with the joint capsule and form a cuff around the head of the humerus. They also create a concavity-compression effect and prevent excessive displacement of the humeral head.
The ligaments and tendons of the shoulder joint are important for the stability of the joint, especially in the extremes of motion. They also provide proprioceptive feedback and sensory information to the joint.
Common Injuries and Conditions
The shoulder joint is susceptible to various injuries and conditions, due to its high mobility and low stability. Some of the common problems that affect the shoulder joint are:
Rotator Cuff Tears
A rotator cuff tear is a partial or complete rupture of one or more of the rotator cuff tendons. It can be caused by acute trauma, such as a fall or a direct blow, or by chronic degeneration, such as overuse or aging. The most commonly affected tendon is the supraspinatus, followed by the infraspinatus, the subscapularis, and the teres minor.
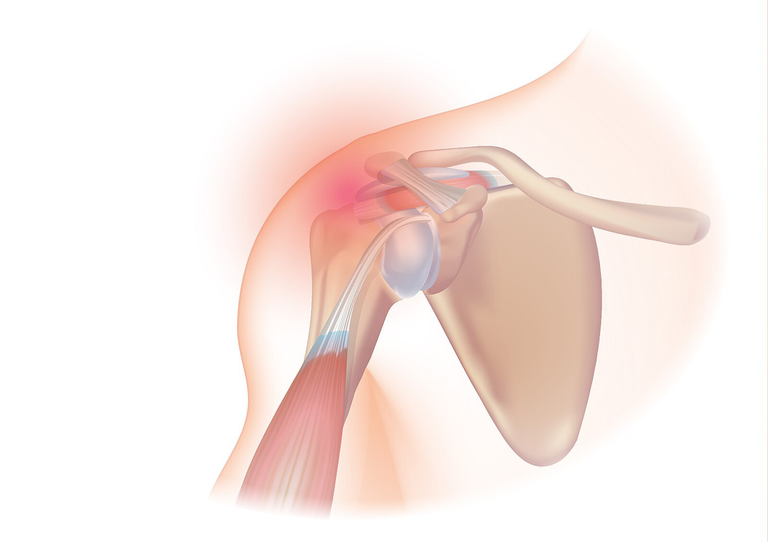
The symptoms of a rotator cuff tear include pain, weakness, and reduced range of motion in the shoulder joint. The pain is usually worse with overhead activities, such as reaching or throwing. The weakness is usually more pronounced in external rotation, abduction, and flexion of the arm. The range of motion is usually limited in all directions, especially in internal rotation and abduction.
The diagnosis of a rotator cuff tear is based on the history, physical examination, and imaging tests, such as X-rays, ultrasound, or MRI. The treatment of a rotator cuff tear depends on the severity, location, and cause of the tear, as well as the age, activity level, and preference of the patient. The treatment options include:
- Non-surgical treatments, such as rest, ice, anti-inflammatory drugs, physical therapy, and corticosteroid injections. These can help reduce pain, inflammation, and improve function in mild to moderate tears.
- Surgical treatments, such as arthroscopic or open repair, debridement, or tendon transfer. These can help restore the integrity, strength, and function of the rotator cuff in severe or chronic tears.
Dislocations and Instability
A dislocation is a condition where the humeral head is completely displaced from the glenoid cavity, resulting in loss of contact between the articular surfaces. An instability is a condition where the humeral head is partially displaced from the glenoid cavity, resulting in excessive movement or laxity of the joint. Both conditions can be caused by acute trauma, such as a fall or a direct blow, or by chronic factors, such as congenital defects, ligamentous laxity, or muscle weakness.
The symptoms of a dislocation or instability include pain, deformity, and reduced range of motion in the shoulder joint. The pain is usually severe and constant, and may radiate to the arm or neck. The deformity is usually visible and palpable, and may vary depending on the direction of the displacement. The range of motion is usually severely limited in all directions, and may be accompanied by crepitus or clicking sounds.
The diagnosis of a dislocation or instability is based on the history, physical examination, and imaging tests, such as X-rays, ultrasound, or MRI. The treatment of a dislocation or instability depends on the type, direction, and frequency of the displacement, as well as the age, activity level, and preference of the patient. The treatment options include:
- Non-surgical treatments, such as closed reduction, immobilization, anti-inflammatory drugs, physical therapy, and bracing. These can help restore the alignment, reduce pain, inflammation, and prevent recurrence in acute or first-time cases.
- Surgical treatments, such as arthroscopic or open stabilization, capsular repair, labral repair, or bone grafting. These can help restore the stability, integrity, and function of the joint in chronic or recurrent cases.
Arthritis
Arthritis is a condition where the articular cartilage of the joint is damaged or worn out, resulting in inflammation, pain, and stiffness of the joint. It can be caused by various factors, such as aging, trauma, infection, autoimmune disorders, or metabolic disorders. The most common types of arthritis that affect the shoulder joint are:
- Osteoarthritis, which is a degenerative condition where the cartilage gradually breaks down due to wear and tear. It usually affects older people and causes pain, stiffness, and reduced range of motion in the shoulder joint. The pain is usually worse with activity and relieved by rest. The stiffness is usually more pronounced in the morning or after periods of inactivity. The range of motion is usually limited in all directions, especially in internal rotation and abduction of the arm.
- Rheumatoid arthritis, which is an inflammatory condition
—
References
(1) The Shoulder Joint - Structure - Movement - TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/joints/shoulder/.
(2) Glenohumeral Joint Anatomy, Stabilizer, and Biomechanics - Shoulder .... https://www.orthobullets.com/shoulder-and-elbow/3032/glenohumeral-joint-anatomy-stabilizer-and-biomechanics.
(3) Glenohumeral (Shoulder) joint: Bones, movements, muscles | Kenhub. https://www.kenhub.com/en/library/anatomy/the-shoulder-joint.
(4) The Shoulder Joint - Structure - Movement - TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/joints/shoulder/.
(5) Glenohumeral (Shoulder) joint: Bones, movements, muscles | Kenhub. https://www.kenhub.com/en/library/anatomy/the-shoulder-joint.
(6) Shoulder Muscles: Anatomy, Function & Common Conditions - Cleveland Clinic. https://my.clevelandclinic.org/health/body/21798-shoulder-muscles.
(7) Anatomy of the Human Shoulder Joint - Verywell Health. https://www.verywellhealth.com/shoulder-anatomy-2549240.
(8) Shoulder | Radiology Reference Article | Radiopaedia.org. https://radiopaedia.org/articles/shoulder.
(6) Nerves of the Shoulder | ShoulderDoc. https://www.shoulderdoc.co.uk/article/1181.
(9) The Intrinsic Muscles of the Shoulder - TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/muscles/shoulder/intrinsic/.
(10) The Shoulder Joint - Structure - Movement - TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/joints/shoulder/.
(11) Glenohumeral (Shoulder) joint: Bones, movements, muscles | Kenhub. https://www.kenhub.com/en/library/anatomy/the-shoulder-joint.
(12) 7.3: Shoulder Joint - Biology LibreTexts. https://bio.libretexts.org/Bookshelves/Human_Biology/Human_Anatomy_Lab/07%3A_Joints/7.03%3A_Shoulder_Joint.
(13) Anatomy of the Shoulder – Edmonton Bone & Joint Centre. https://edmontonboneandjoint.ca/services/shoulder/anatomy-of-the-shoulder/.
(14) The Anatomy of the Shoulder - Washington University Orthopedics. https://www.ortho.wustl.edu/content/Patient-Care/3127/Services/Shoulder-Elbow/Overview/Shoulder-Arthroscopy-Information/The-anatomy-of-the-shoulder.aspx.


Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider delegating to the @stemsocial account (85% of the curation rewards are returned).
You may also include @stemsocial as a beneficiary of the rewards of this post to get a stronger support.
Dear @jsalvage !
Thank you for good article!
I appreciate your time reading the article.
How are you doing
Dear James!
I am fine thank you and you?
I have seen news reports that the current political and economic situation in Nigeria is not very good.
I pray for your health and happiness!